What RadCall does
Increase efficiency, throughput, and clinical impact day or night
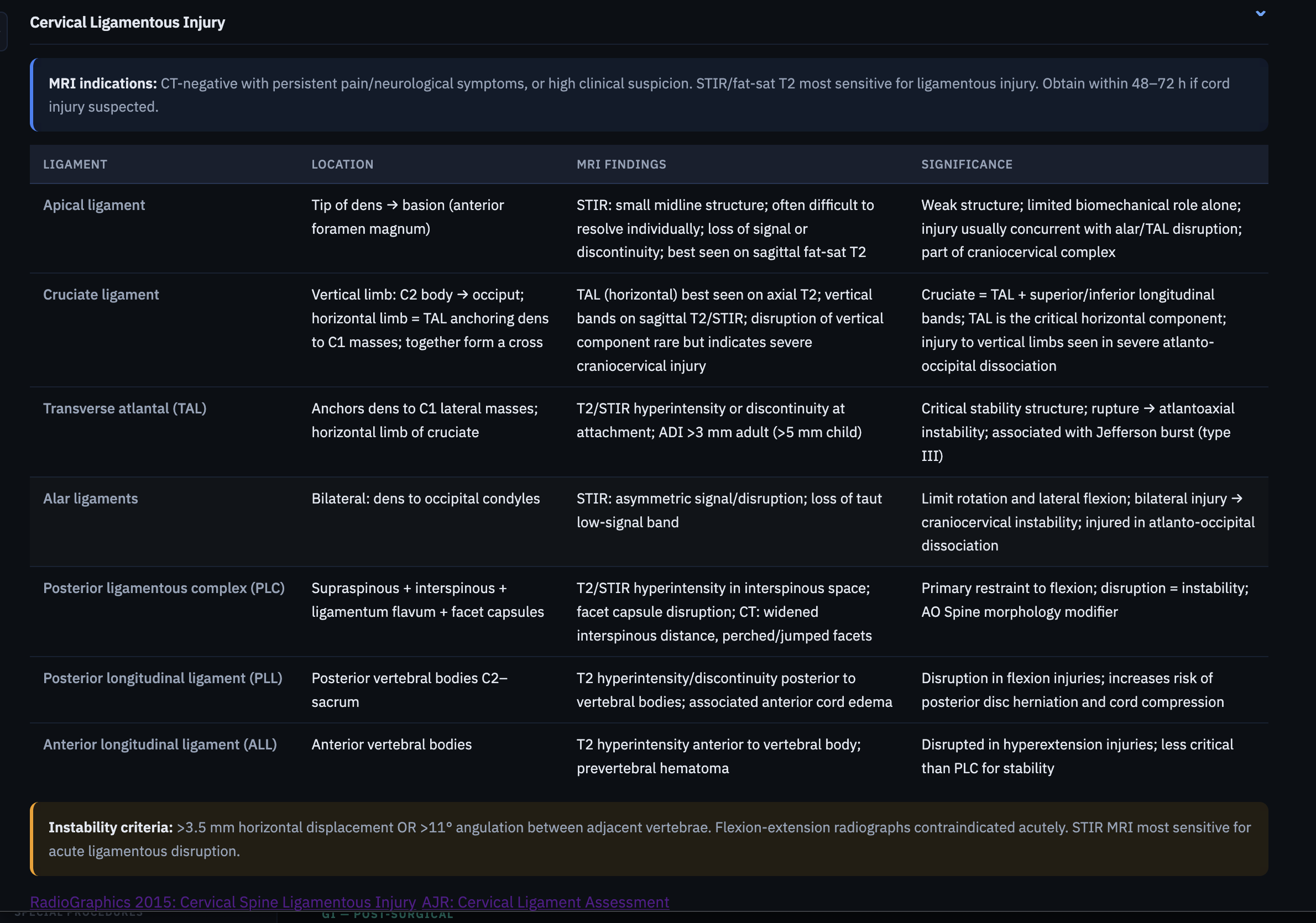
Clinical Guides
Every guide you need, structured for speed
Anatomy, grading scales, reporting frameworks, and differentials — organized for rapid review when you're at the workstation, not a textbook.
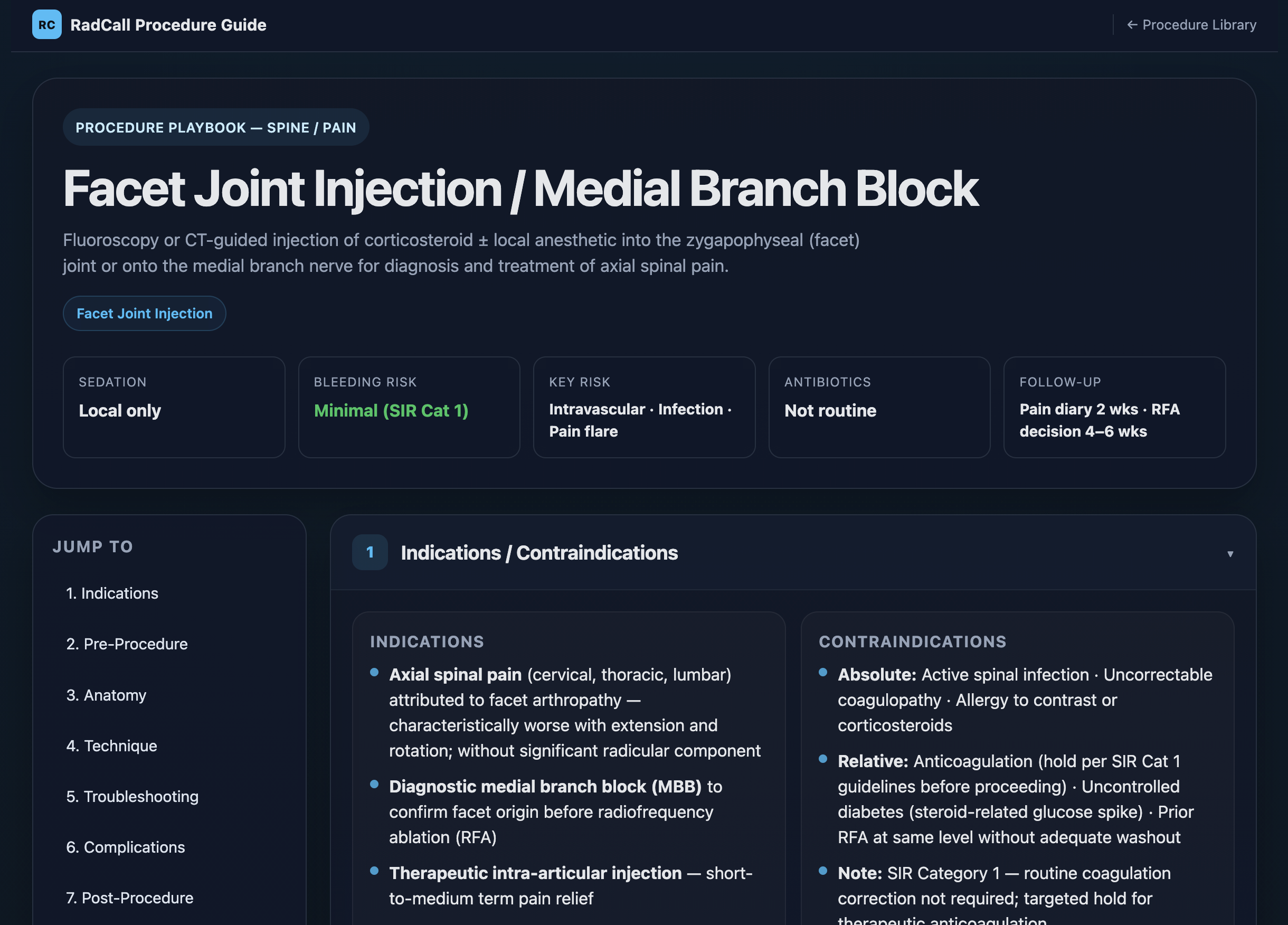
IR Procedure Playbooks
99+ procedures, step-by-step
Technique, setup, sedation, bleeding risk, key complications, and periprocedural management. Everything you need before you scrub — from paracentesis to TIPS.
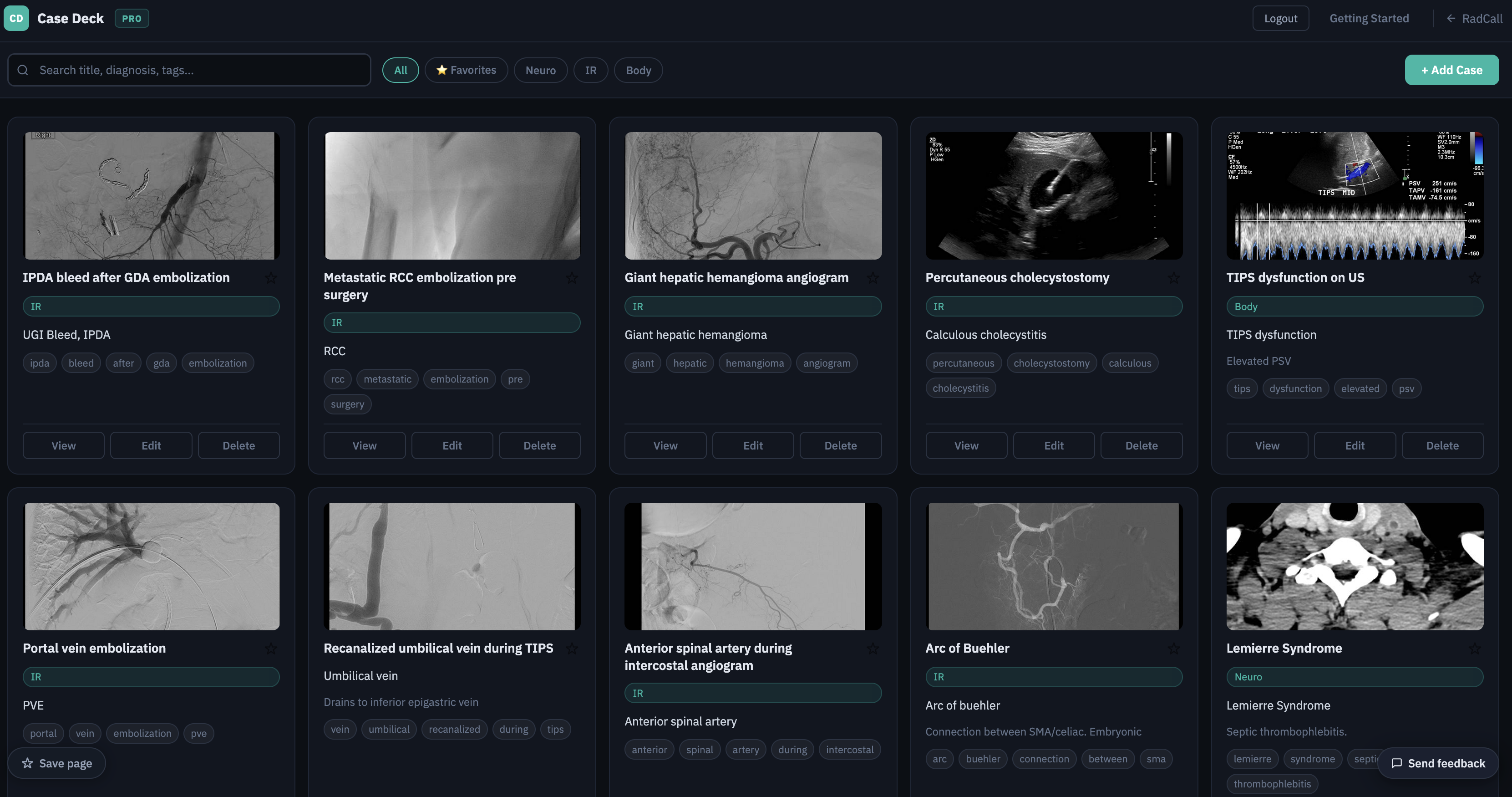
Workflow Tools
Track productivity, cases, and procedures
Case deck, procedure log, and wRVU tracking — built for residents building their case collection and attendings tracking productivity alike.
See it in action
Watch demos