Table of Contents
- General resources
- Normal shoulder measurements
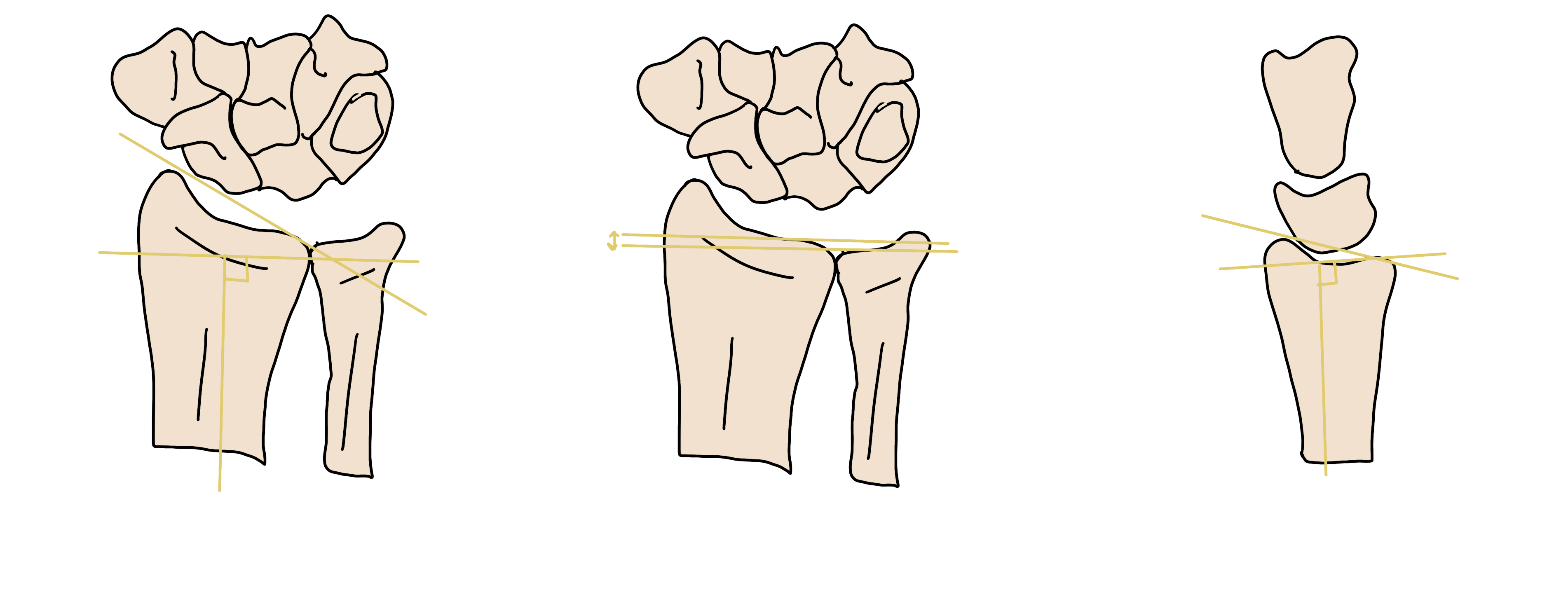
- Lateral wrist anatomy
- Wrist ligaments
- Ankle ligaments
- Pelvic radiograph search pattern
- Proimal femur anatomy
MSK Trauma Quick Reference Guides
- Hand and Wrist
- Elbow
- Distal Humerus
- Proximal Humerus
- Clavicle
- Scapula
- Pelvic
- Acetabulum
- Proximal Femur
- Knee
- Mid Tibia/Fibula
- Ankle
- Foot
For spine imaging please see the neuroradiology section.
GENERAL RESOURCES
- Atlas of Normal Variants
- Atlas of Orthopedic Hardware by Location
- Normal for Age by Gender
- Upper Extremity Trauma
- Lower Extremity Trauma
- Pelvis and Hip Trauma
- Bone Tumor Identification (Stanford)
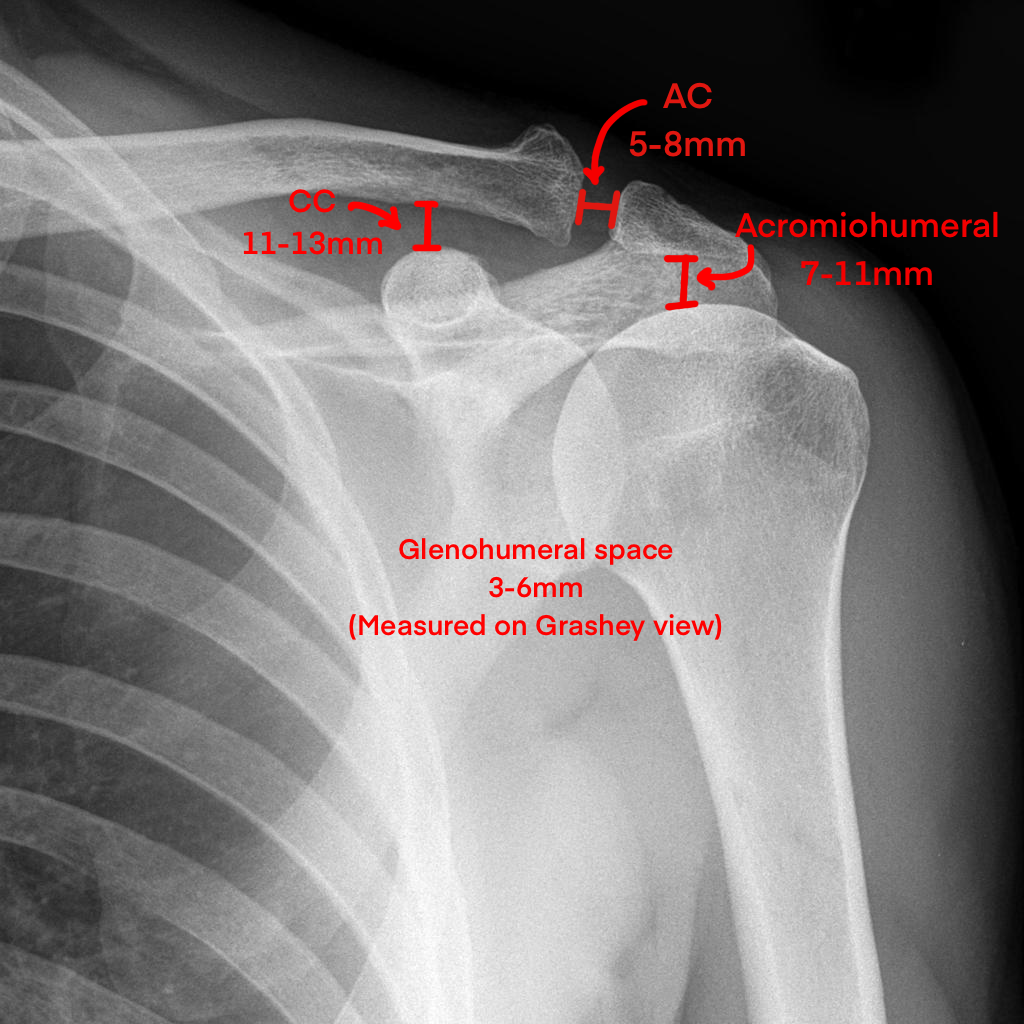
NORMAL SHOULDER MEASUREMENTS
Lateral Wrist Bony Anatomy

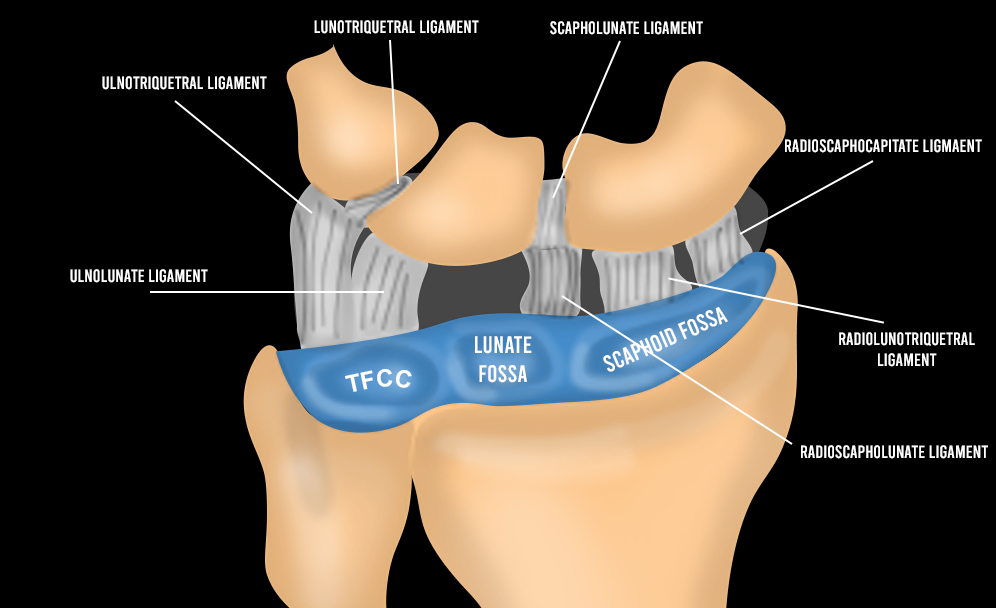
Wrist Ligaments
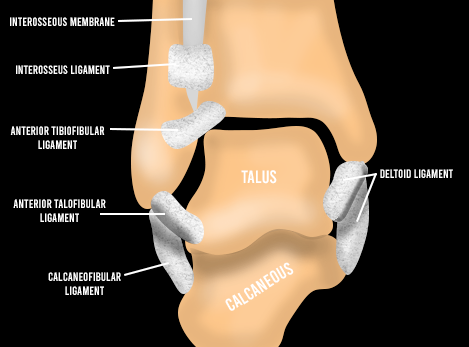
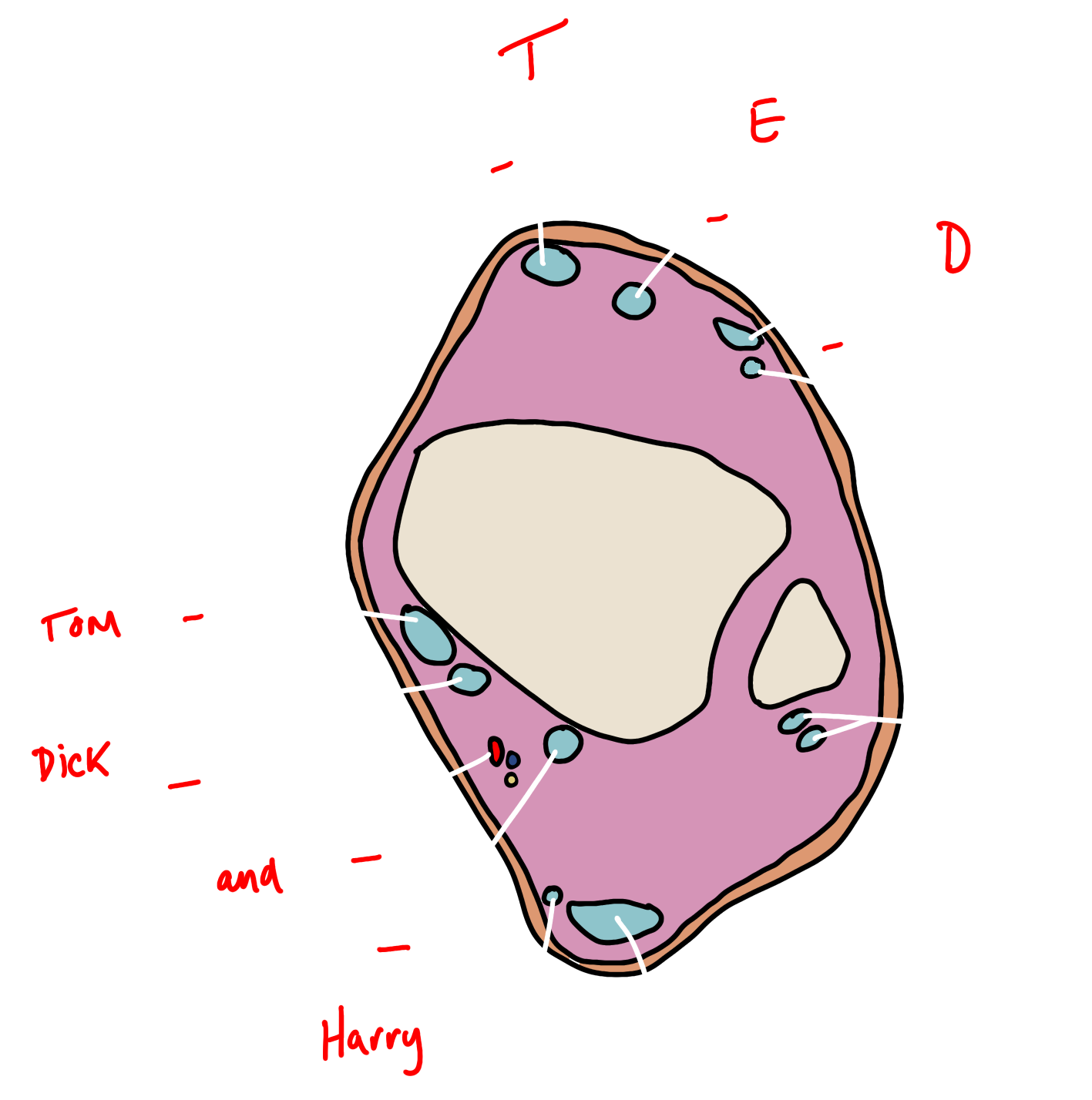
Ankle Ligaments
PELVIC RADIOGRAPH SEARCH PATTERN


Proximal Femur Anatomy

HAND AND WRIST
Hand


WRIST
Distal Radius Fractures
Reporting Checklist
- Loss of volar tilt
- Loss of radial inclination
- Shortening of the radius relative to the ulna
- Intraarticular extension
- Diastasis or depression at the intraarticular fracture site
- Comminution
- Associated ulnar styloid fracture
- Location and degree of displacement
- If styloid base fracture, is the DRUJ and TFCC intact
- Disruption of the carpal arcs
Named Fractures
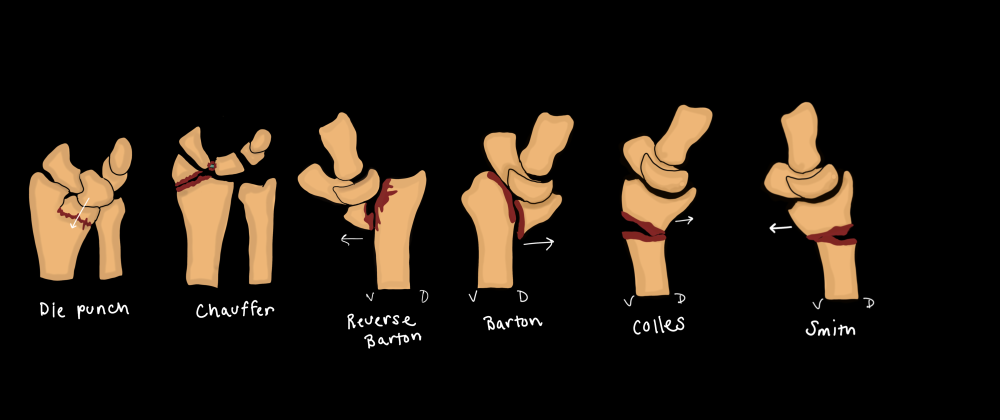
- Just describe the fracture, don’t use eponyms
Galeazzi Fracture-Dislocation
Reporting Checklist
- Description of radial fracture
- Degree of shortening
- DRUJ dislocation direction

- Fracture of the distal radius with dislocation of the DRUJ
- Classification
- Type I: dorsal displacement of the distal radius
- Type II: volar displacement of the distal raidus
Essex-Lopresti fracture-dislocation
- Fracture of the radial head with dislocation of the DRUJ and rupture of the interosseous membrane
ELBOW
Radial Head Fractures
Reporting Checklist
- Degree of displacement
- Amount of articular surface involved (%)
- Presence of comminution or dislocation
Mason-Johnston Classification
- Type 1 – No or minimal (<2mm) displacement
- Type 2 – Displacement >2mm, >30% <50% articular surface involvement
- Type 3 – Comminution of the radial head without dislocation
- Type 4 – Comminution and dislocation of the radial head
Elbow Dislocation
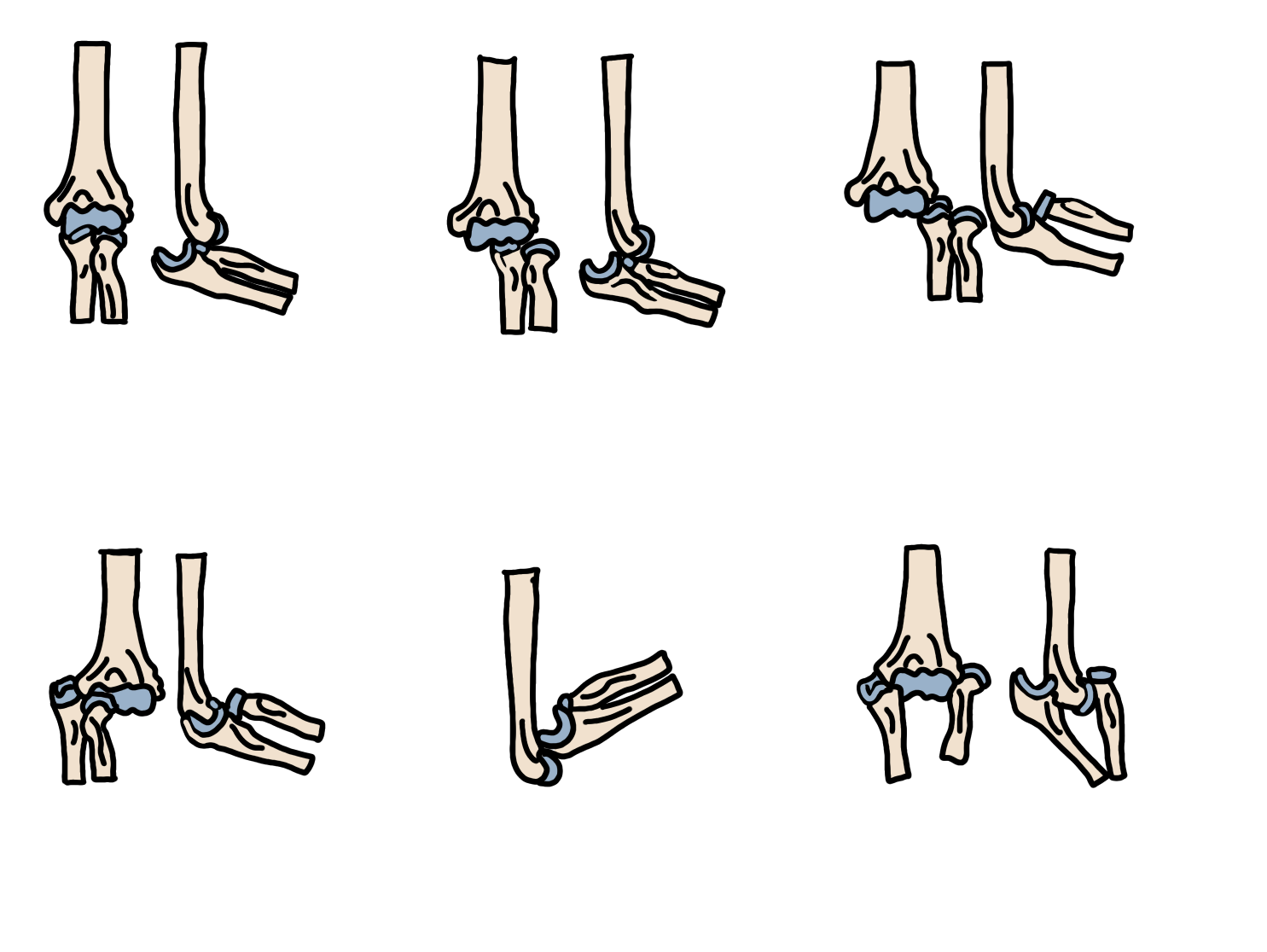
- Posteriolateral most common
- Complex = dislocation + fracture
- Associated fractures
- Medial epicondyle
- Radial head/neck
- Coronoid process
- Terrible triad – get CT if 2/3 seen to exclude the third injury
- Posterior elbow dislocation
- Radial head fracture
- Coronoid process fracture
Stages of Dislocation

- Stage 1 – Damage to lateral ligamentous structures (LUCL, RCL)
- Posterolateral rotary instability
- Stage 2 – Capsular and lateral soft tissue damage
- Trochlea is perched on the coronoid process
- Stage 3 – Vary degrees of damage to medial structures (anterior bundle MCL) with frank dislocation
Monteggia Fracture Dislocation
- Ulnar fracture with proximal radius dislocation
- All will go to surgery
Bado Classification
- Type 1 – Most Common – Anterior angulation of the ulnar fragment apex with anterior dislocation of the radius
- Type 2 – Posterior fracture angulation of the ulna and radial head
- Type 3 – Pediatrics – Ulnar metaphyseal fracture with lateral dislocation of the radial head
- Type 4 – Fracture of the proximal radius and ulna

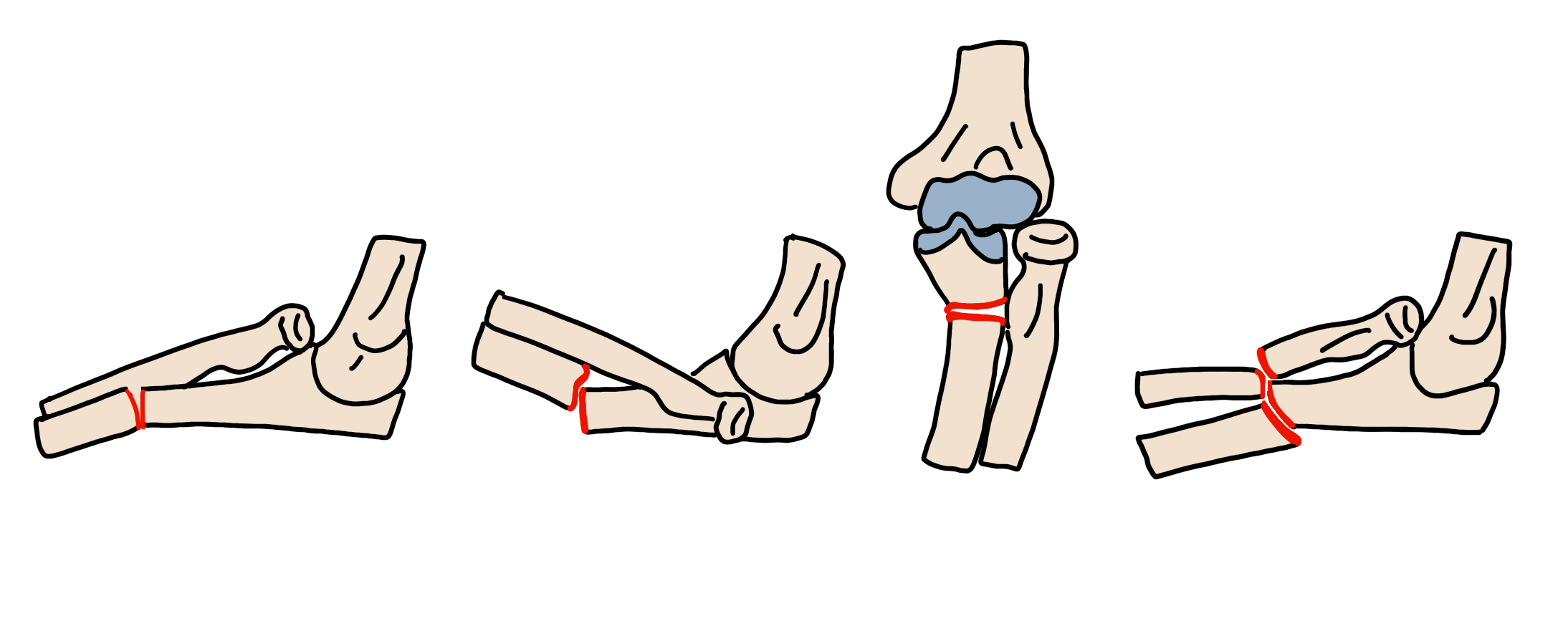
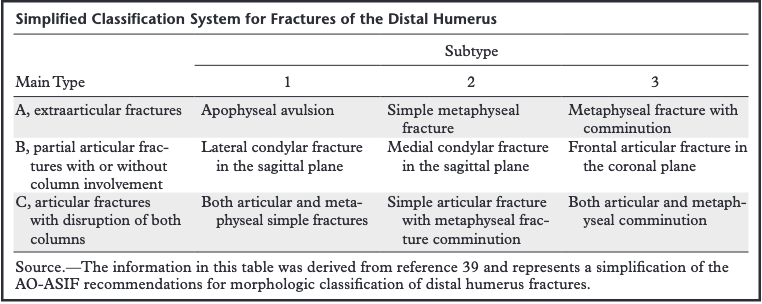
DISTAL HUMERUS
Reporting Checklist
- Column involvement – medial or lateral
- Direction and degree of displacement of epicondylar avulsion fractures and single column fractures
- Presence of comminution or two column injury
Classification System
Coronoid Process Fractures
Classification System
- Type 1 – Transverse tip fracture
- Type 2 – Anteromedial facet involvement – MCL injury
- Type 3 – Base of coronoid process (>50% disruption)

Olecranon Fractures
Reporting Checklist
- Degree of displacement
- >2mm displacement = surgery
- Presence of comminution
- Comminution = surgery
Mayo Classification System
- Type 1 – Non-displaced
- Type 2- Intact MCL, displaced >3mm
- Type 3 – Displaced, unstable

PROXIMAL HUMERUS
Reporting Checklist

- Typically do not list the parts since the ortho may disagree
- Part = >1cm displacement or 45 degree angulation
CLAVICLE
Clavicle Fracture
Reporting Checklist
- Fracture location along the shaft (lateral third, middle third, medial third)
- Angulation and fracture end displacement (including direction)
- Comminution
- Degree of overlap
- Acromioclavicular and sternoclavicular joint integrity
- Coracoclavicular distance
In general, if >100% displacement will be managed operatively
Rockwood Classification of Acromioclavicular Joint Injury
| Type I | Clavicle not elevated relative to the acromion |
| Type II | Clavicle elevated but not above the superior border of the acromion |
| Type III | Clavicle elevated above the superior border of the acromion CC distance is less than twice normal (<25 mm) |
| Type IV | Clavicle displaced posterior into the trapezius |
| Type V | Clavicle is elevated and CC distance is more than double normal (>25 mm) Consider weight-bearing projections |
| Type VI | Rare; clavicle inferiorly displaced behind coracobrachialis and biceps tendons |
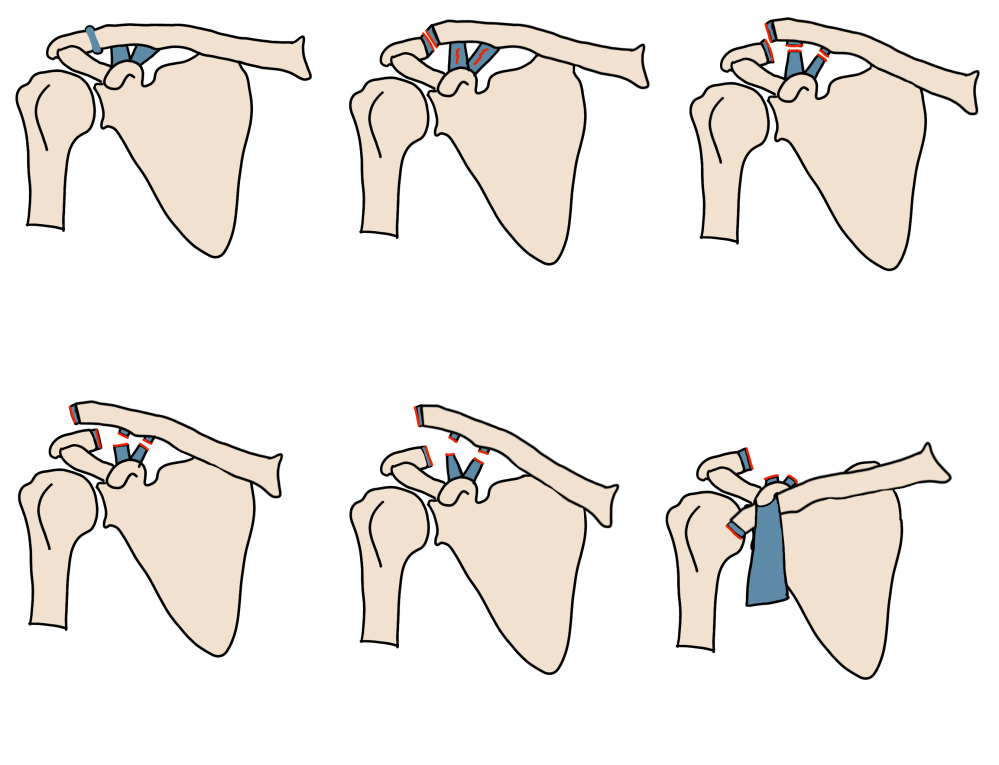
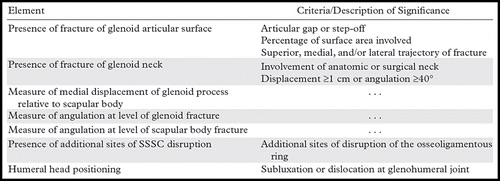
SCAPULA
Reporting Checklist
Commonly involves:
- Scapular body
- Acromion
- Coracoid process
- Glenoid neck or articular surface (requires surgical repair)
Superior Suspensory Complex – support complex of the shoulder. Disruption of any two = unstable injury requiring surgery. Disruption of three = floating shoulder (high energy trauma)

- Glenoid process
- Coracoid process
- Coracoclavicular ligament
- Distal end of the clavicle
- Acromioclavicular joint
- Coracoacromial ligament
- Acromial process
Scapular Neck Fracture Classification

- Type 1 – Nonangulated, nondisplaced
- Type 2a – Shortened or displaced > 1 cm
- Type 2b – Angulated > 40 degrees
Ideberg Classification of Glenoid Fossa Fractures

| Type 1a | Anterior rim |
| Type 1b | Posterior rim |
| Type 2 | Transverse to lateral margin |
| Type 3 | Transverse to superior margin |
| Type 4 | Transverse to medial margin |
| Type 5a | Transverse lateromedial |
| Type 5b | Transverse superomedial |
| Type 5c | Transverse superomediolateral |
| Type 6 | Comminuted crush |
PELVIC FRACTURES
Stable Pelvic Fractures
- Isolated pubic ramus of ischium fracture
- Unilateral fractures of both rami
- Isolated sacral fractures (usually transverse)
- Avulsion fractures
- Duverney fracture – peripheral fracture to the iliac wing (associated with ileus)


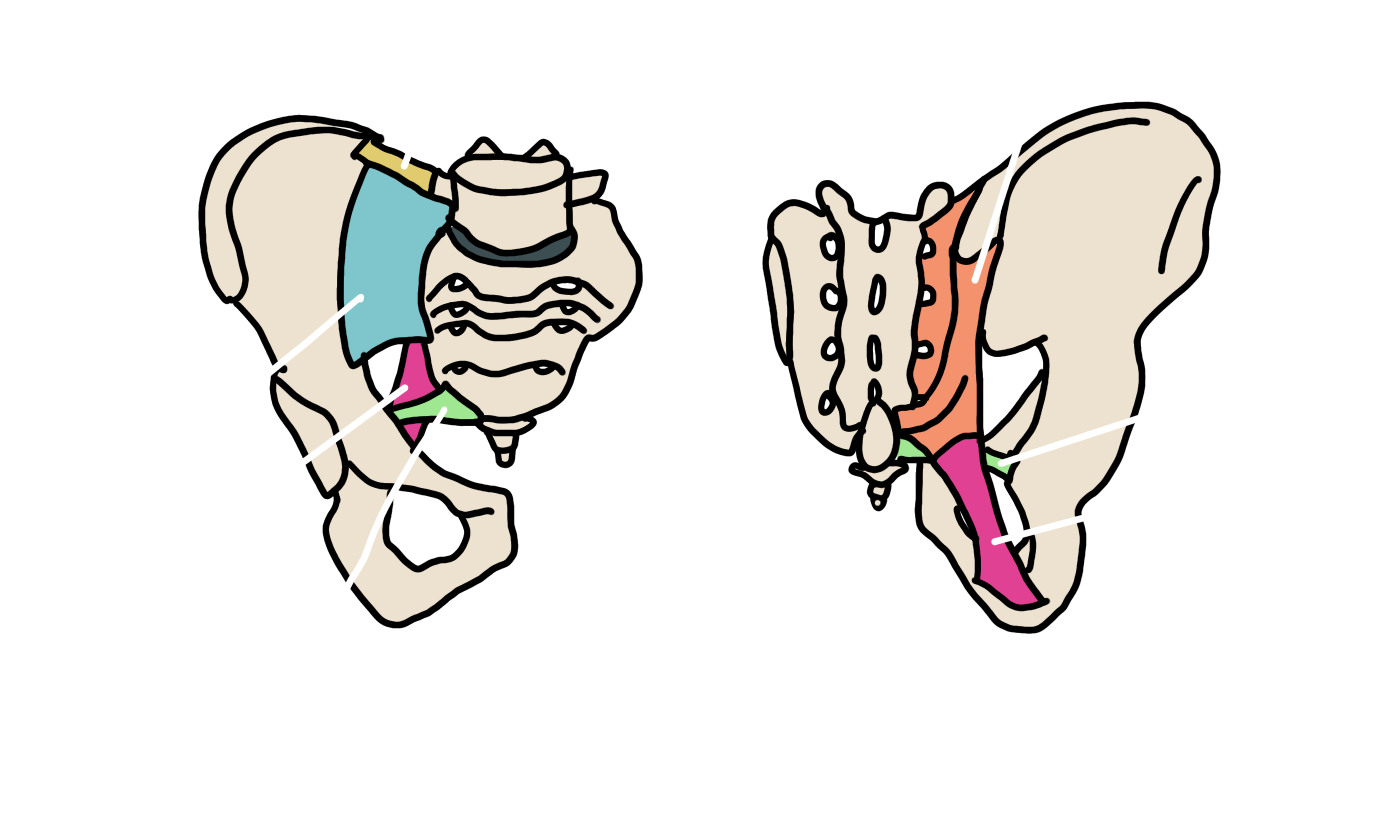
Pelvic Ligaments
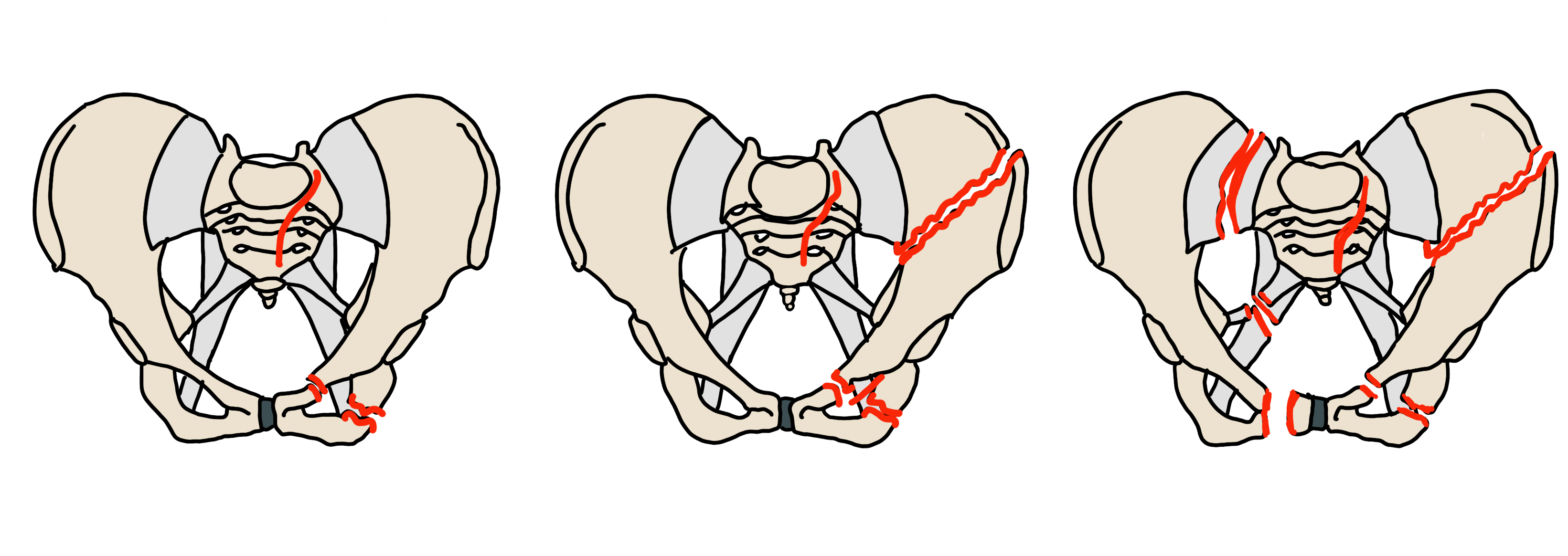
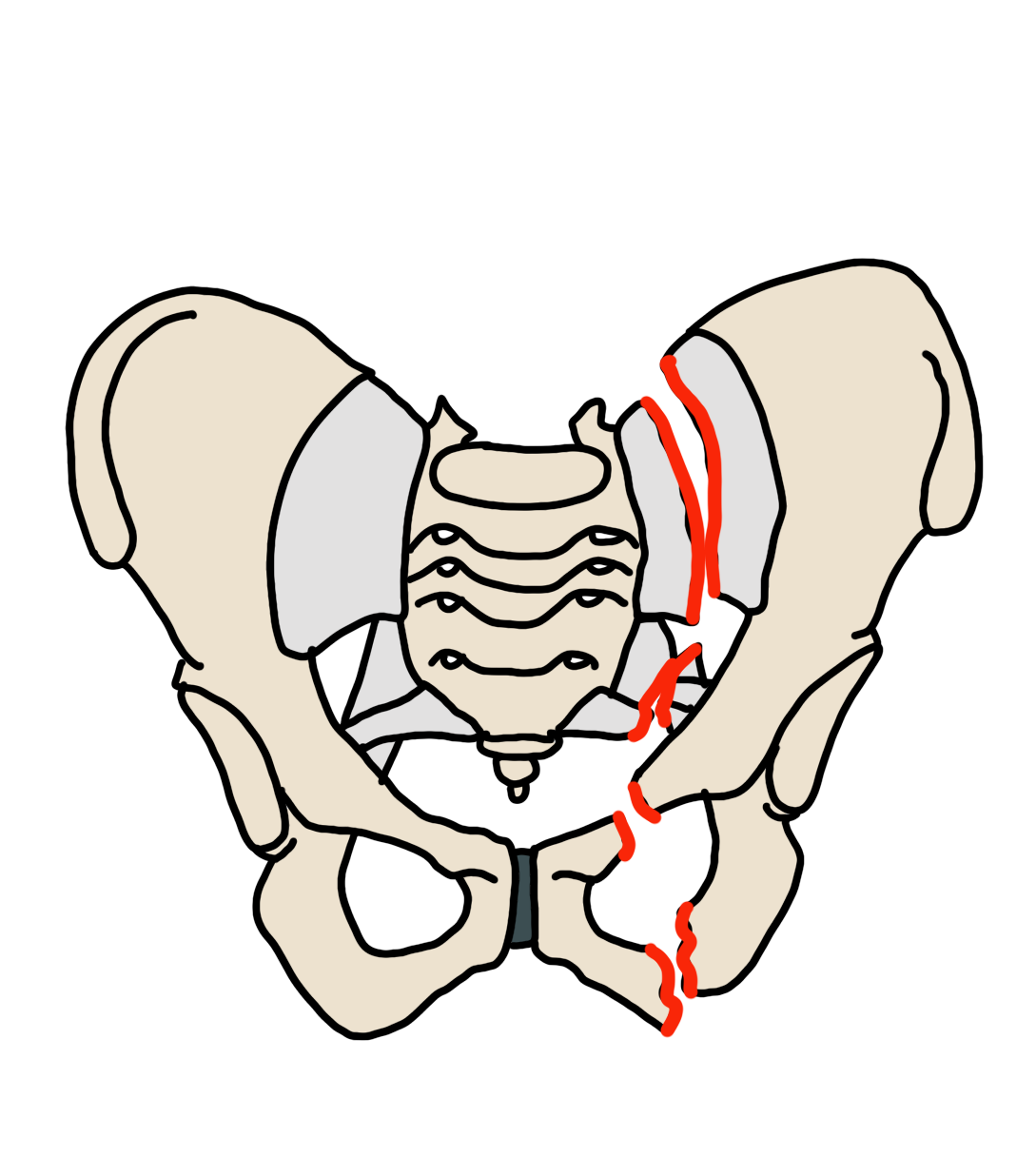
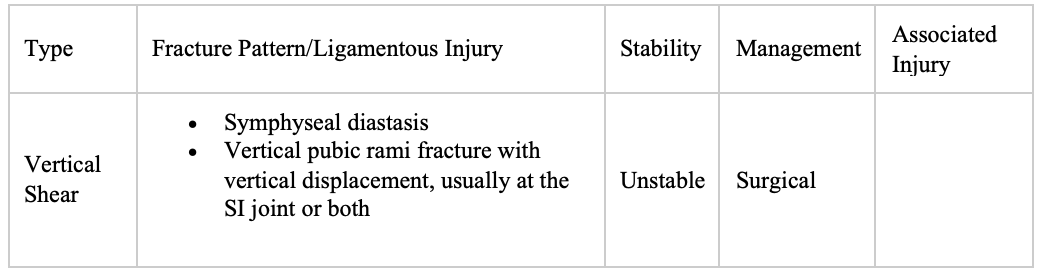
Young and Burgess Classification of Pelvic Ring Fractures



ACETABULAR FRACTURES
Anatomy

Judet and Letournel classification of Acetabular Fractures
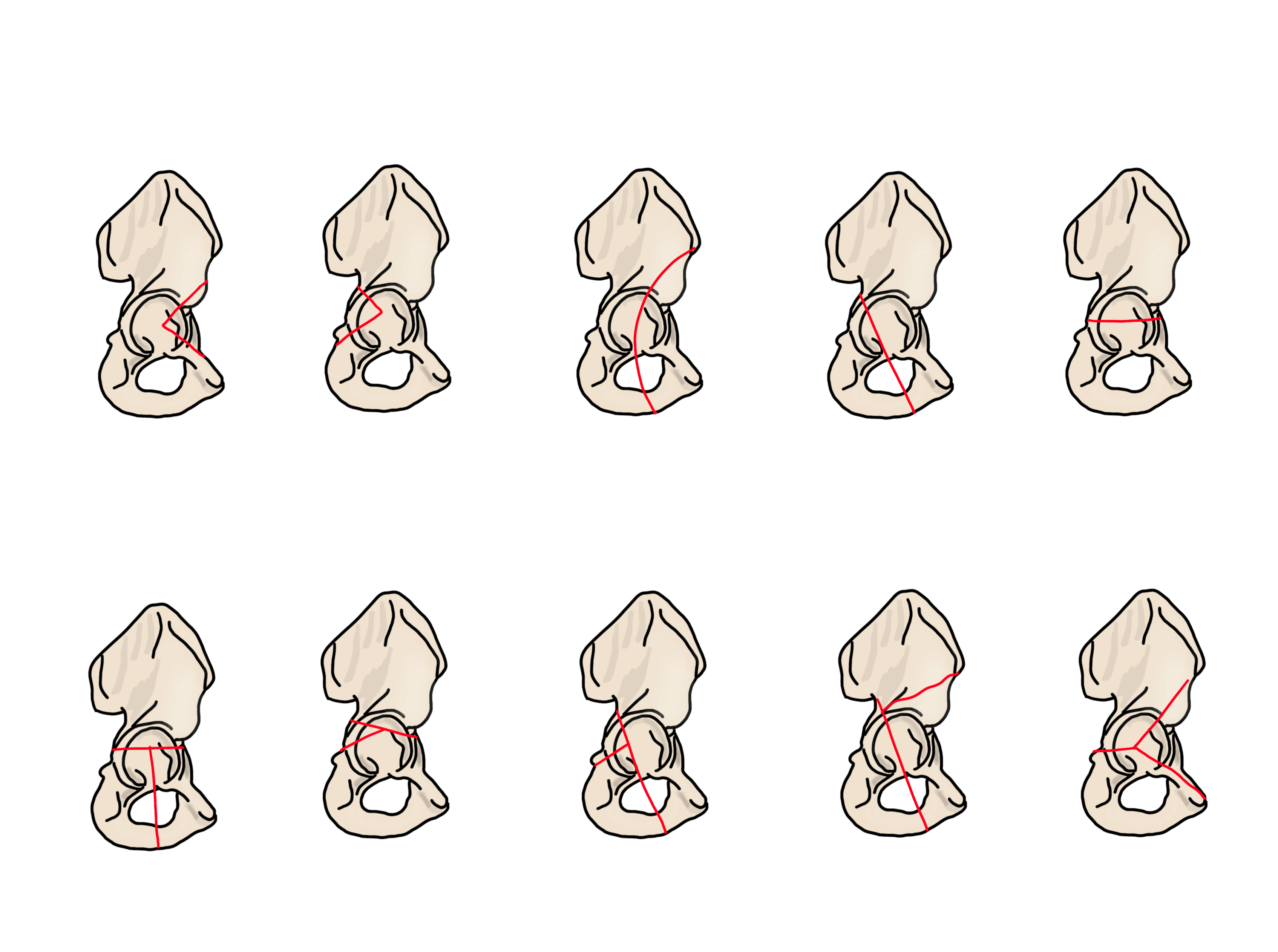
Anterior Column – Pelvic brim, anterior wall, superior pubic ramus, anterior iliac wing
Posterior Column – Greater and lesser sciatic notch, posterior wall, ischial tuberosity

PROXIMAL FEMUR FRACTURES
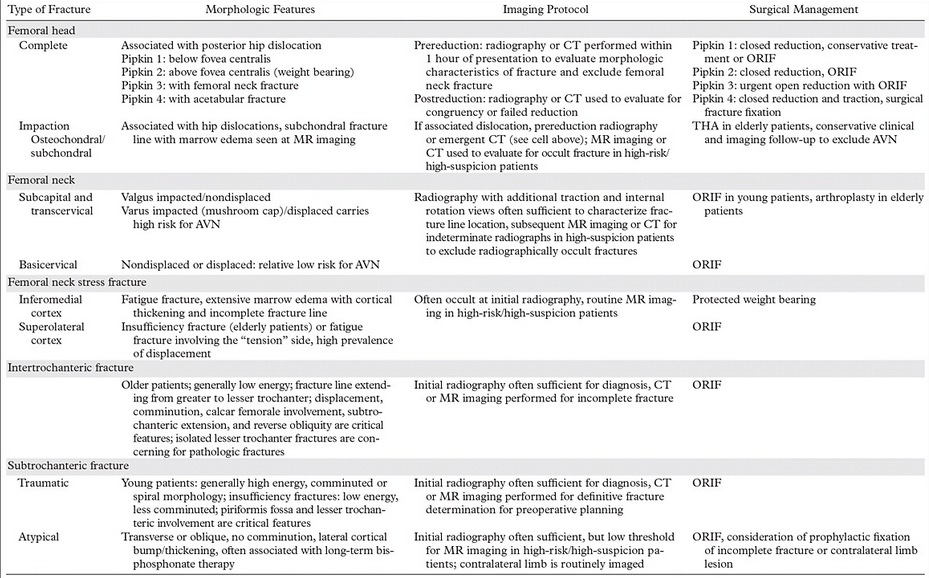
Types of Fractures
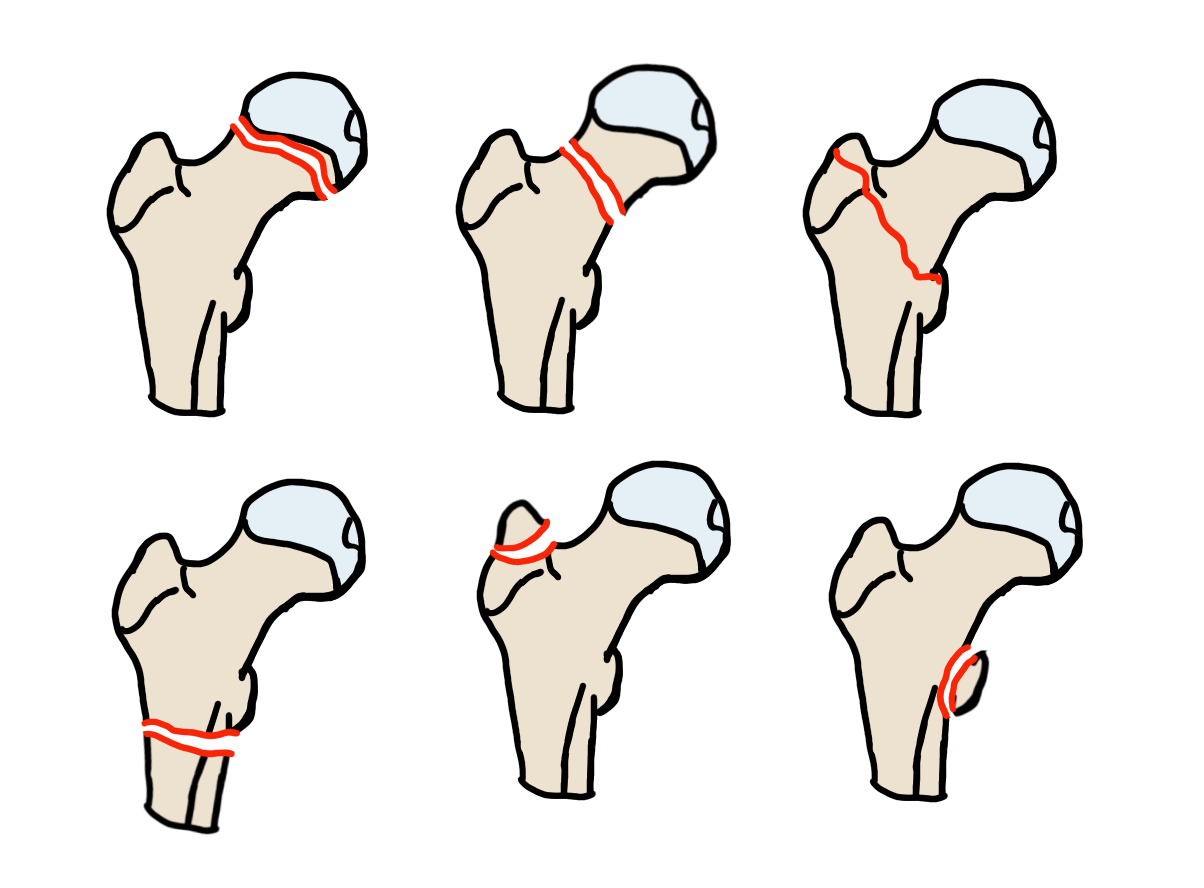
Intracapsular Fractures
Pipkin Classification of Femoral Head Fractures
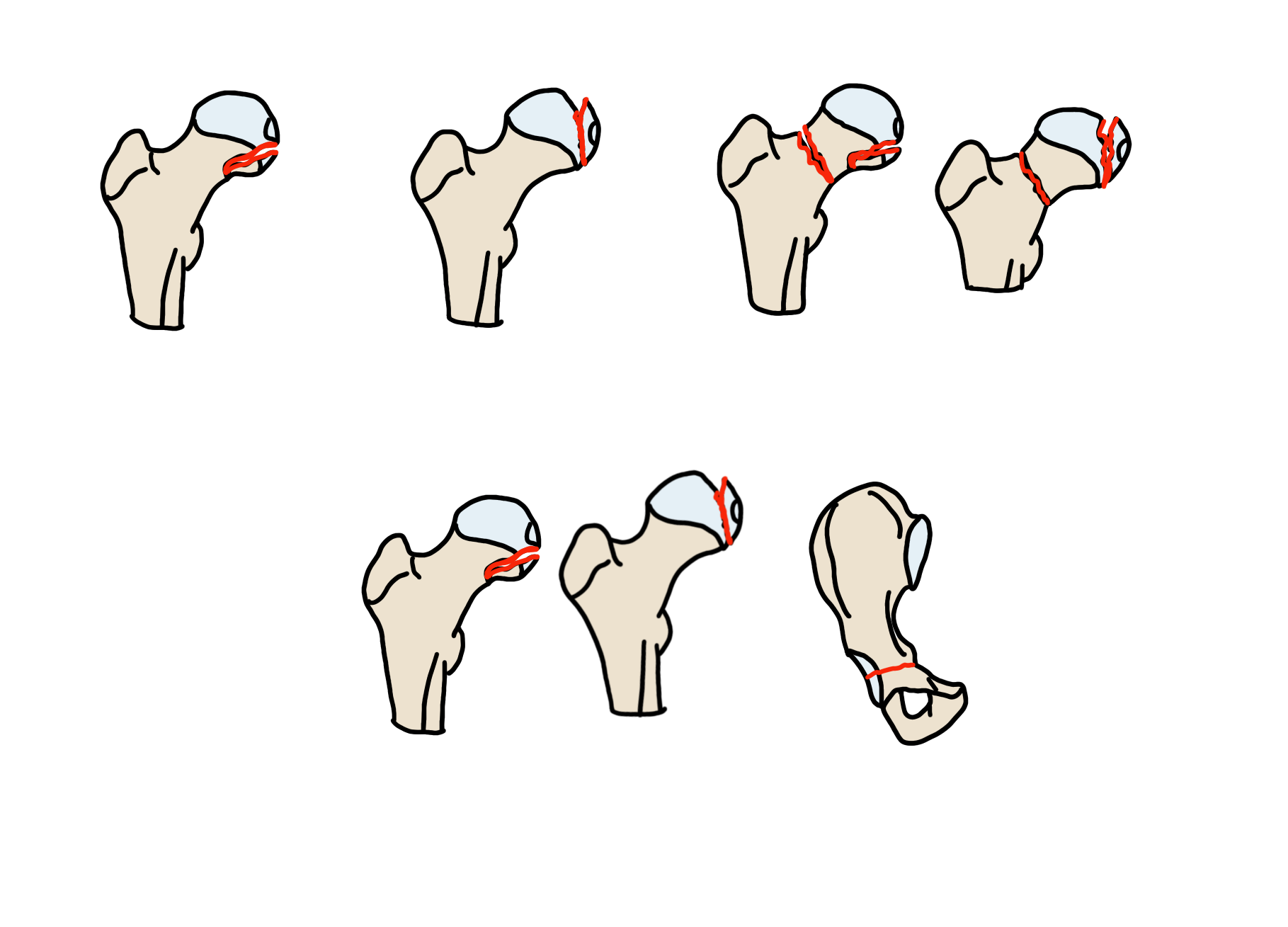
| Type | Characteristics |
| Type I | Inferior to the fovea centralis |
| Type II | Superior to the fovea centralis |
| Type III | Combination of type I/II with femoral neck fracture |
| Type IV | Combination of type I/II with acetabular fracture |
Dislocation
Reporting Checklist
- Type of dislocation
- Posterior > anterior
- Associated femoral neck fracture
- Reduction is contraindicated with coexisting femoral neck fracture
- Associated femoral head impaction fracture
- More common with anterior dislocation
- Requires THA
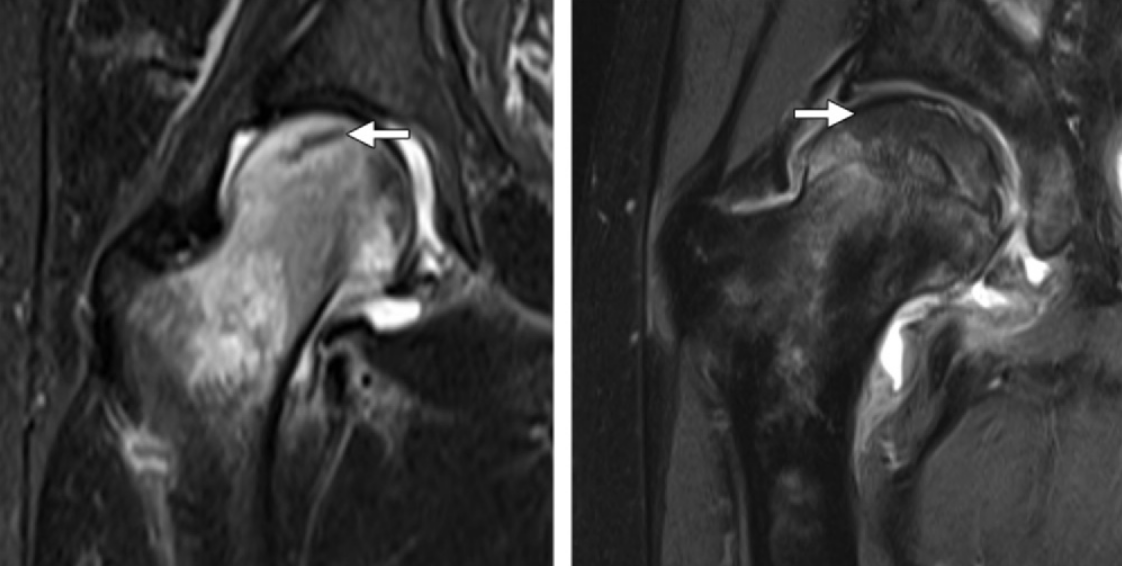
Femoral Neck Fractures
Reporting Checklist
- Location
- Subcapital
- Transcervical
- Basicervical
- Displaced or nondisplaced
- If elderly – Garden Classification – the worse grade the higher risk of AVN
Garden Classification of Femoral Neck Fractures
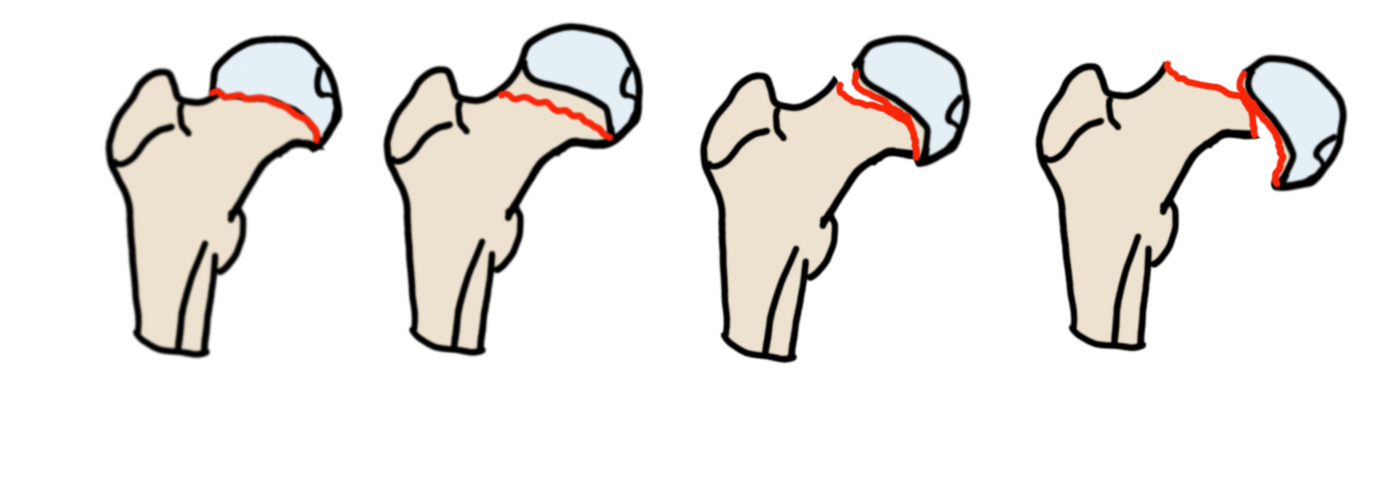
| Type | Characteristics |
| Type 1 | Incomplete or valgus impacted |
| Type 2 | Complete, nondisplaced |
| Type 3 | Complete, partially displaced |
| Type 4 | Complete, fully displaced |
Extracapsular Fractures
Intertrochanteric Fractures
Reporting Checklist
- Involvement of the posteromedial cortex
- If intact = stable
- If involved = unstable
- Reverse fracture – unstable
- Subtrochanteric extension – unstable
Evan-Jensen Classification of Intertrochanteric Fractures

| Type | Characteristics | Stability |
| Type I | Two-part nondisplaced fracture | Stable |
| Type II | Two-part minimally displaced fracture | Stable |
| Type III | Three-part with loss of posterolateral support | Stable |
| Type IV | Three-part with loss of posteromedial support | Unstable |
| Type V | Four-part with loss of both posteromedial and lateral support | Unstable |
| Type R | Reverse obliquity fracture | Unstable |
Lesser Troachanter Fracture – if isolated think malignancy
Subtrochanteric Fractures
- High rate of complications
- Trauma – comminuted fractures
- Elderly – spiral fractures
- Bisphosphonate therapy
- Transverse (primarily); medially may be oblique
- Lateral cortex, medial spike if complete fracture
- No or minimal comminution
- Endosteal or periosteal thickening
Seinsheimer Classification of Subtrochanteric Fractures

| Type | Characteristics |
| Type 1 | Any fracture with <2mm displacement |
| Type 2A | Two-part transverse fracture |
| Type 2B | Two-part spiral fracture with the lesser trochanter in the proximal fragment |
| Type 2C | Two-part spiral fracture with the lesser trochanter in the distal fragment |
| Type 3A | Three-part spiral fracture, the third fragment is the lesser trochanter |
| Type 3B | Three-part fracture with third part a butterfly fragment |
| Type 4 | Four or more fragments |
| Type 5 | Any fracture with extension into the greater trochanter |
KNEE
- Distal femur fractures
- Fibular fractures
- Patellar fractures
- Plain film signs of ligamentous injury
- Tibial fractures
- Dislocation
- Proximal tibiofibular joint dislocation
Distal Femur Fractures
Reporting Checklist
- Fracture fragments
- Articular or extraarticular
- If articular measure the articular surface step-off
- Presence of floating knee – extra-articular fractures of the proximal tibia and distal femur
- If fracture recommend inmaging of the proximal femur and hip
- If posterior displocation – recommend CTA to evaluation popliteal injury
AO/OTA Classification of Distal Femur Fractures

| Type | Characteristics |
| A1 | Simple, nondisplaced |
| A2 | Metaphyseal wedge |
| A3 | Complex metaphyseal |
| B1 | Sagittal fracture of the lateral condyle |
| B2 | Sagittal fracture of the medial condyle |
| B3 | Coronal fracture of one or both condyles (Hoffa fragment) |
| C1 | Simple articular and metaphyseal |
| C2 | Comminuted metaphyseal component with simple articular componenet |
| C3 | Comminuted articular and metaphyseal components |
Fibular Fractures
Reporting Checklist
- Location of fracture (fibular head, avulsion, fibular shaft)
- Fibular head fracture – asociated with peroneal nerve injury and foot drop
- Also association with posterolateral corner injury and instability
- Fibular shaft fracture – Recommend imaging of ankle to exclude a Maisonneuve fracture
- Fibular head fracture – asociated with peroneal nerve injury and foot drop
- Degree of subluxation
- Anterolateral
- Posteromedial
- Superior
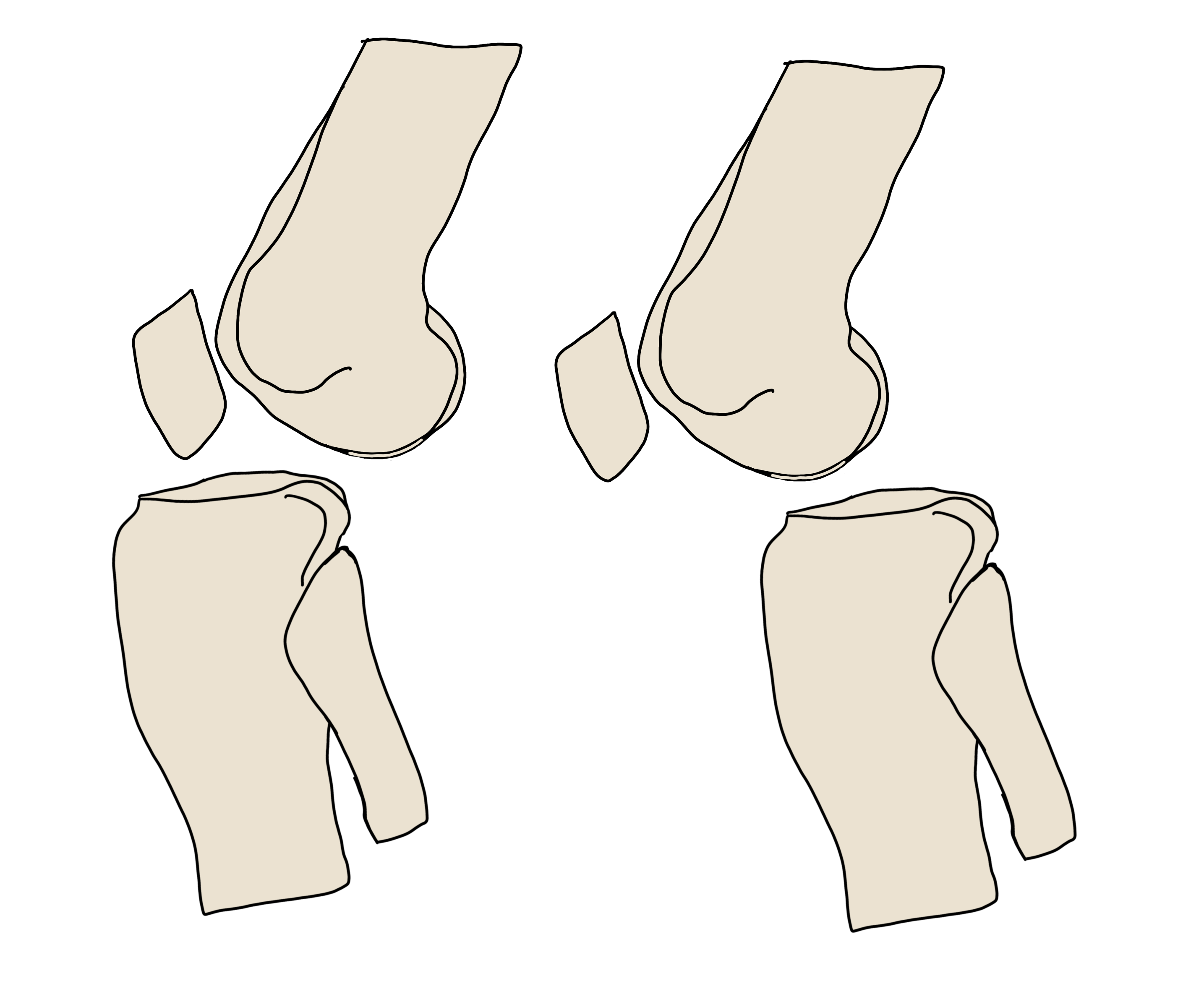
Patellar Fractures
- Transverse fracture most common
- Sugical management
- >2mm incongruity at articular surface
- >3mm separation of fracture fragments
- Disruption of extensor mechanism

AO/OTA Classification of Patellar Fractures

Plain Film Signs of Ligamentous Injury
- Tibial spine avulsion fracture – associated with MCL and medial meniscus injury
- Can be isolated and cause knee instability
- If seen – recommend MRI
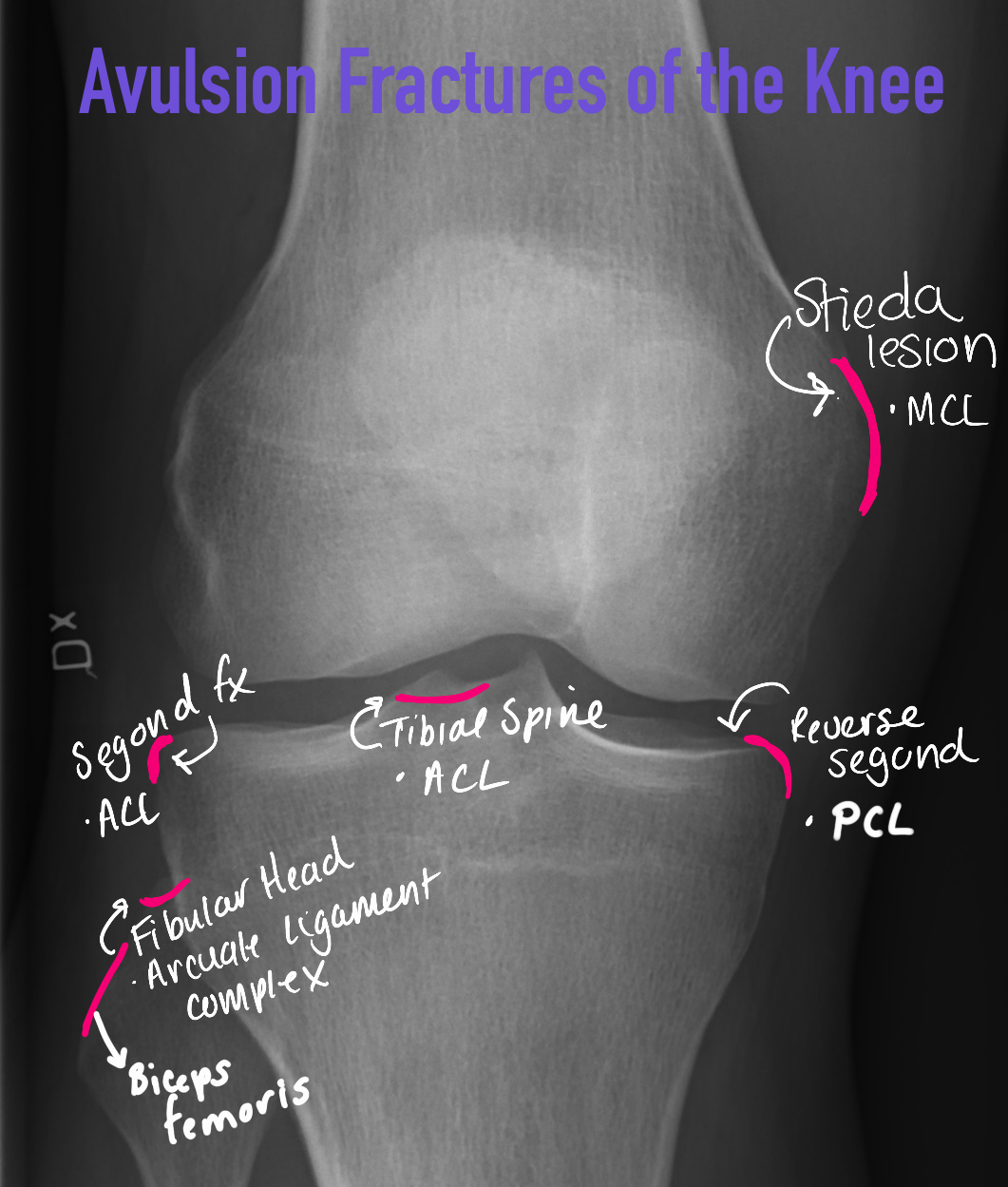
Deep Notch Sign – impaction fracture of the lateral femoral condyle associated with ACL injury

Tibial Fractures
Reporting Checklist
- Size, number and location of fracture fragments and fracture lines
- Presence of contralateral joint space widening
- Split, depressed, or bicondylar morphology
- Nonsurgical management if diastasis <3-4 mm and depression <4-5mm
Schatzker Classification of Tibial Plateau Fractures

| Type | Characteristics |
| Type I | Split fracture with no depression |
| Type II | Lateral split fracture with depression of the weight bearing portion |
| Type III | Focal depression of articular surface without split |
| Type IV | Medial plateau fracture |
| Type V | Bicondylar split fracture +/- depression |
| Type VI | Bicondylar split fracture with dissocation of the metaphysis from diaphysis by transverse fracture component |
Knee Dislocation
- Based on the direction of the tibia
- Anterior most common
- Posterior – dashboard injury
- Can have medial or lateral as well as rotary dislocation
- All should undergo vascular imaging to evaluate for popliteal injury
Proximal Tibiofibular Joint Dislocation
Ogden Classification of PTFJ Dislocation

| Type | Characteristics | Notes |
| Type I | PTFJ subluxation | |
| Type II | Anterolateral | Most common |
| Type III | Posteromedial | Associated with peroneal nerve injury (foot drop) |
| Type IV | Superior | Associated with fracture/dislocation of ankle or distal tibia |
MID TIBIA/FIBULA
Reporting Checklist
- Simple, complex, or wedge
- Shortening or distraction
- Presence of intercalated fragment
AO/OTA Classification
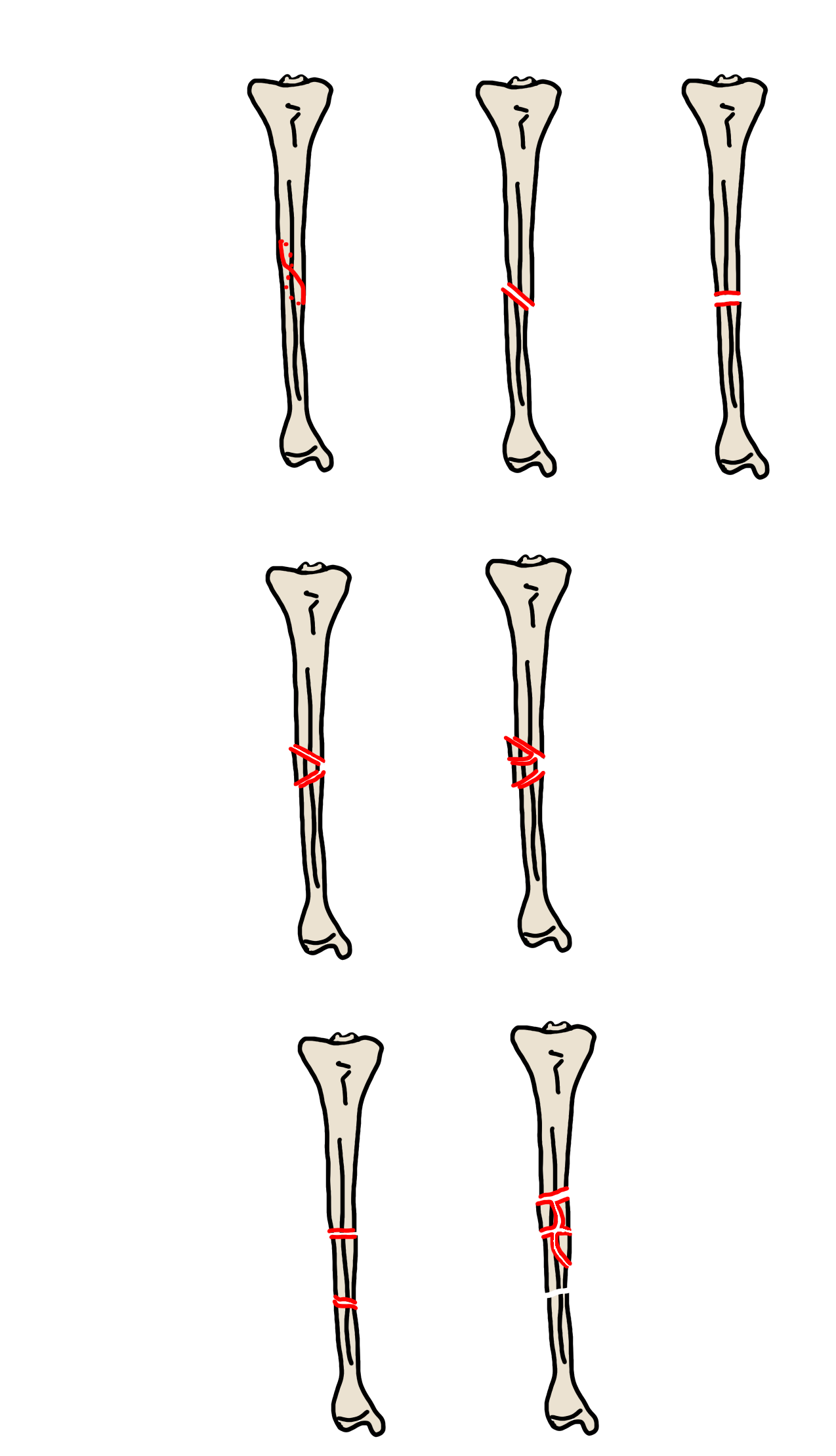
- Similar schema for fibular fractures
- Butterfly fragment – triangular comminuted fragment of bone that does not involve the entire circumference of the shaft
- Ring butterfly fragment – involved entire circumference of shaft
- Bayonet apposition – overriding fracture fragments
- Segmental fracture – intercalated fragment with impaired vasculartity
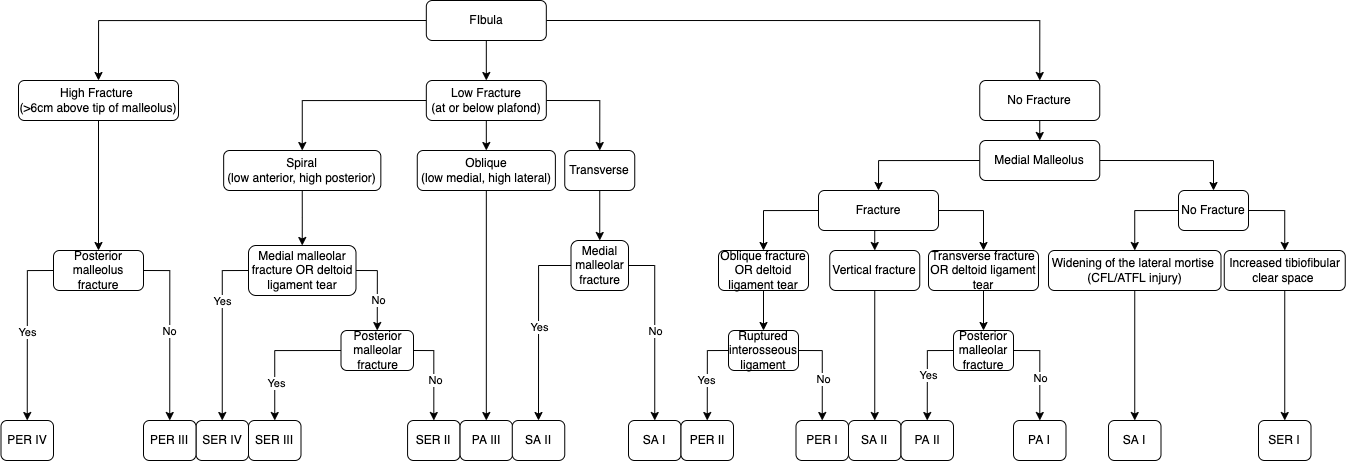
ANKLE FRACTURES
Reporting Checklist
- Fractures – level and pattern
- Ligaments – lateral medial clear space
- Weber/Lauge-Hansen – look for missed injury based on classification
- Dislocation
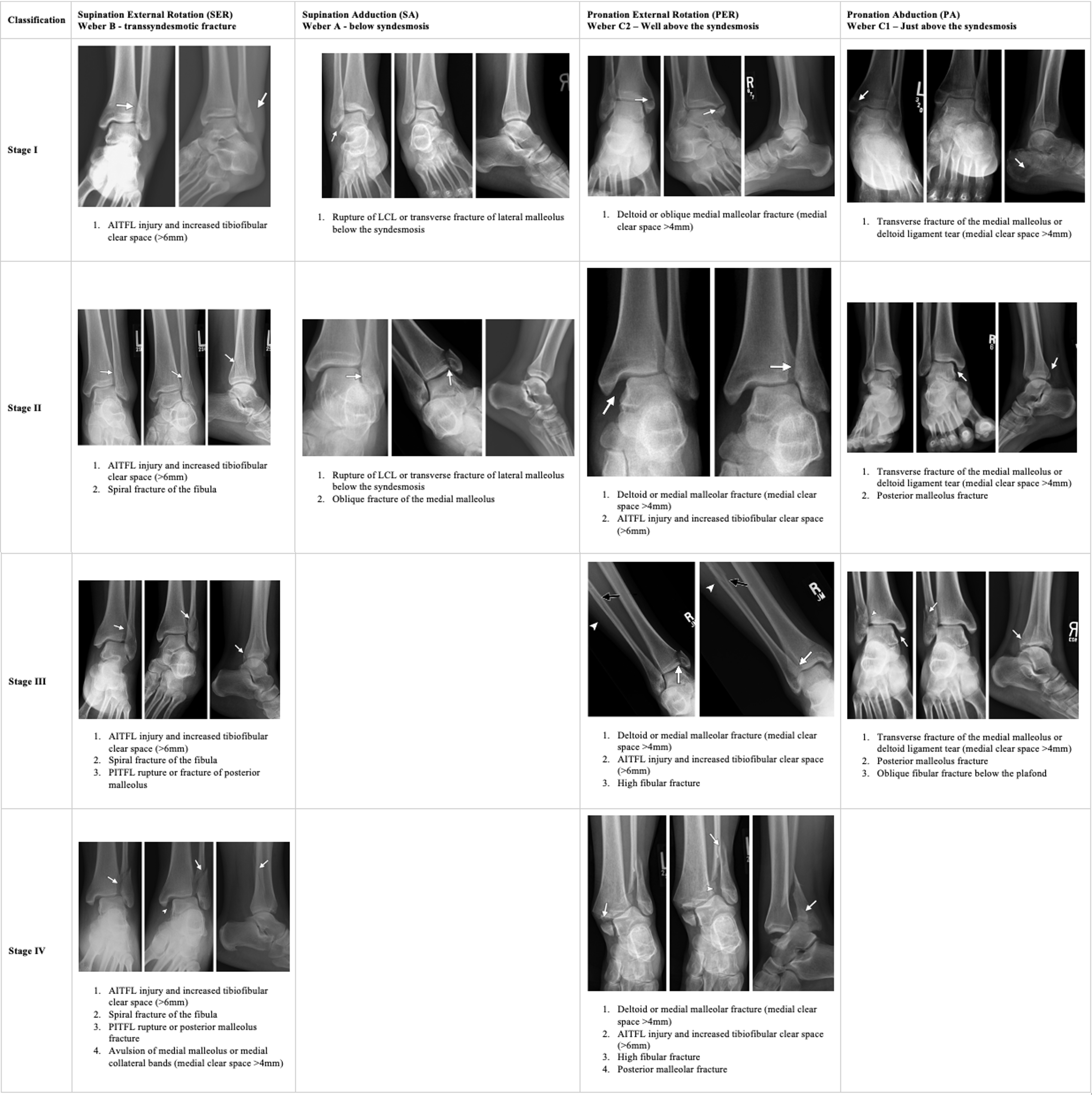
Lauge-Hansen Classification of Ankle Fractures
Tibial Plafond Fractures
Reporting Checklist
- Number and location of major fragments at the level of the articular surface
- Degree and location or articular depression
- >2-3mm is considered significant
- Associated tendon injury or entrapment
- Disruption of the syndesmosis
- Bony fragments in the syndesmosis
- Retinaculum injury

Ruedi and Allgower Classification of Pilon Fractures

| Type | Characteristics |
| Type I | Cleavage fracture with no major articular disruption |
| Type II | Displaced fracture with minimal impaction or comminution |
| Type III | Displaced fracture with significant articular surface comminution and metaphyseal impaction |
FOOT
Talus
Talar Body Fractures
Sneppen Classification of Talar Body Fractures

| Type | Characteristics |
| A | Compression or osteochondral dome fracture |
| B | Coronal shear fracture |
| C | Sagittal shear fracture |
| D | Posterior tubercle fracture |
| E | Lateral tubercle fracture |
| F | Crush comminuted fracture |
Talar Process Fractures
Posterior Process Fracture (Shepard Fracture) – Mimics Os Trigonum

Posteromedial Tubercle Fracture (Cedell Fracture)

Lateral Process Fracture
Reporting Checklist
- Hawkins classification
- Degree of displacement
- >2mm = ORIF
- Largest fracture fragment size
- >1cm can undergo fixation, smaller may need to be excised
Hawkins Classification of Lateral Process Fractures
| Type | Characteristics |
| Type I | Most common – simple fracture with a single fracture line extending from the talofibular articulation to the subtalar joint |
| Type II | Comminuted fracture involving the entire lateral process and both articular surfaces |
| Type III | Only involves the subtalar joint at the anterior-inferior portion of the posterior articular process |
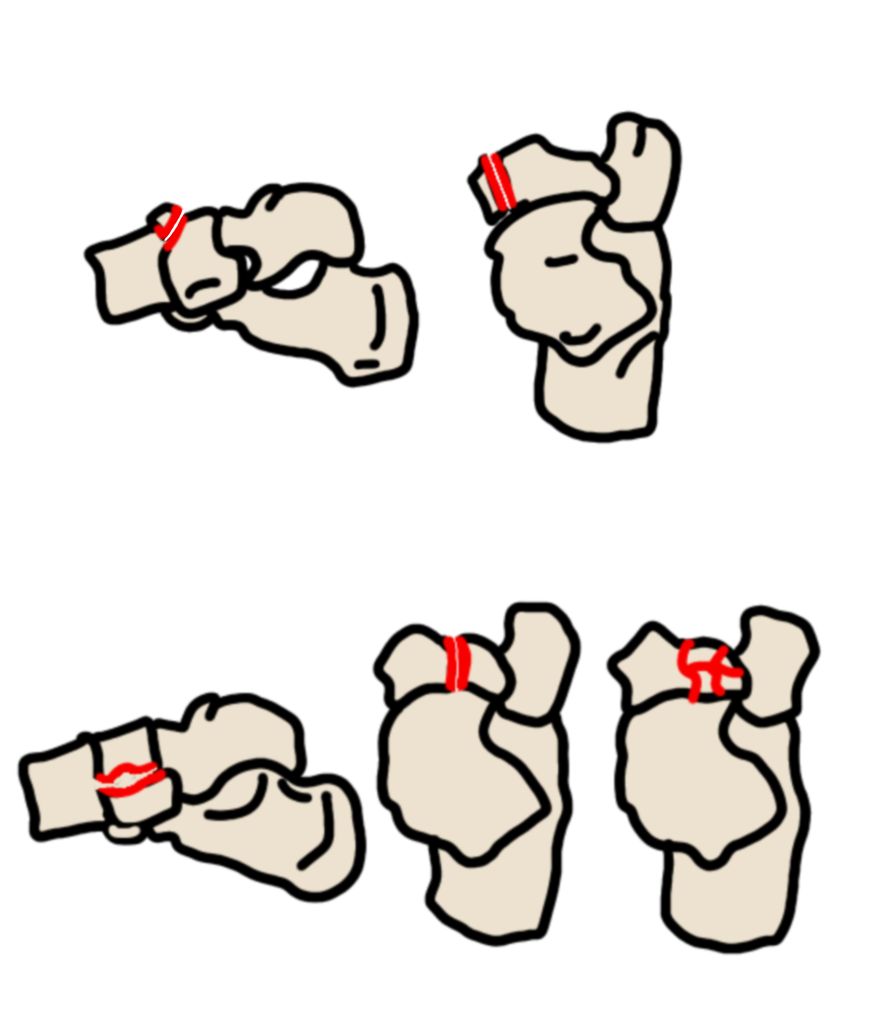
Talar Neck Fracture
Hawkins-Canale Classification of Talar Neck Fractures
| Type | Characteristics | Risk of osteonecrosis |
| Type I | Nondisplaced talar neck fracture | ~10% |
| Type II | Talar neck fracture and talocalcaneal dislocation | ~30% |
| Type III | Talar neck fracture, talocalcaneal dislocation, and tibiotalar dislocation | >90% |
| Type IV | Talar neck fracture, talocalcaneal dislocation, tibiotalar dislocation, talonavicular dislocation | >90% |
Talar Head Fractures
- Least common fracture of the talus
- Fracture of the articular surface of the talus at the talonavicular articulation – associated with dislocation
- Recommend CT to evaluate for extension to talar neck, also associated with midfoot fractures
- Hawkin sign – lucent band parallel to subchondral bone plate of talar dome due to hyperemia
- If seen – osteonecrosis will not develop
- 4-9 weeks after fracture

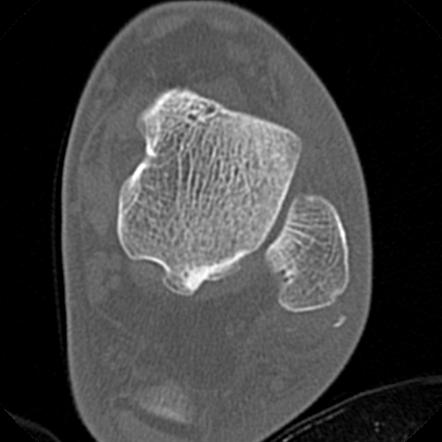
Calcaneal Fractures
Reporting Checklist
- Look for cortical fragments entrapped between dominant fragments – can impede reduction
- Extension into calcaneocuboid joint
- Number of sagittal fracture lines entering the posterior subtalar joint
- Degree of depression of articular fragments
- Look for peroneal retinaculum avulsion
- Look for peroneal tendon entrapment
- Fragments inferior to sustentaculum tali – may entrap flexor hallicus longus tendon, tibial nerve
- Sanders classification
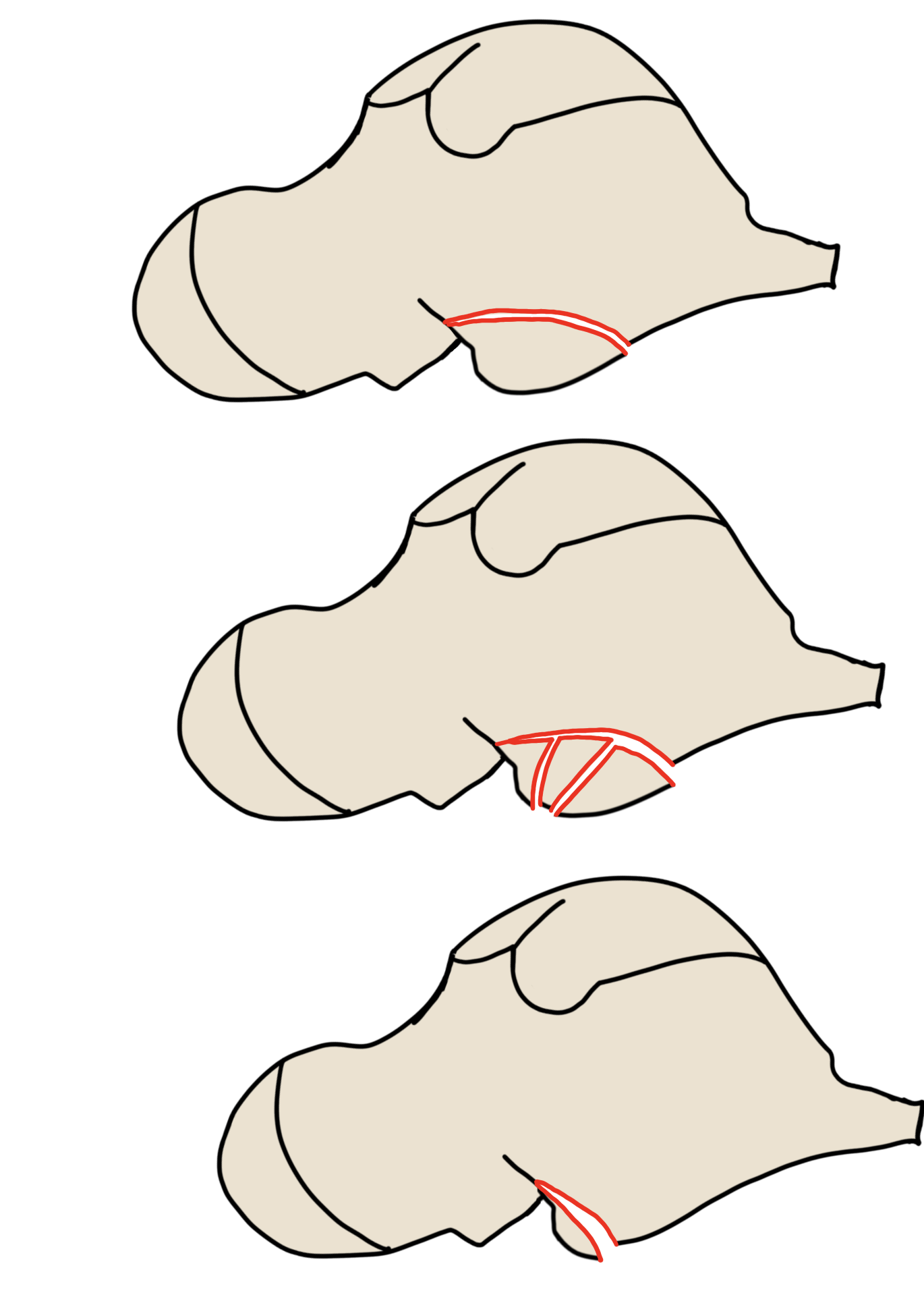
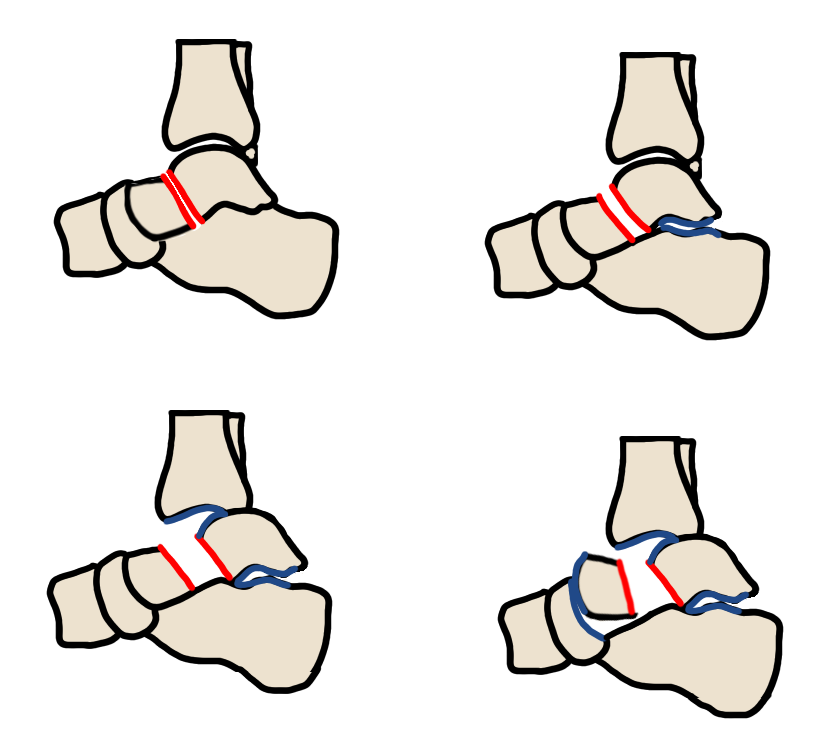
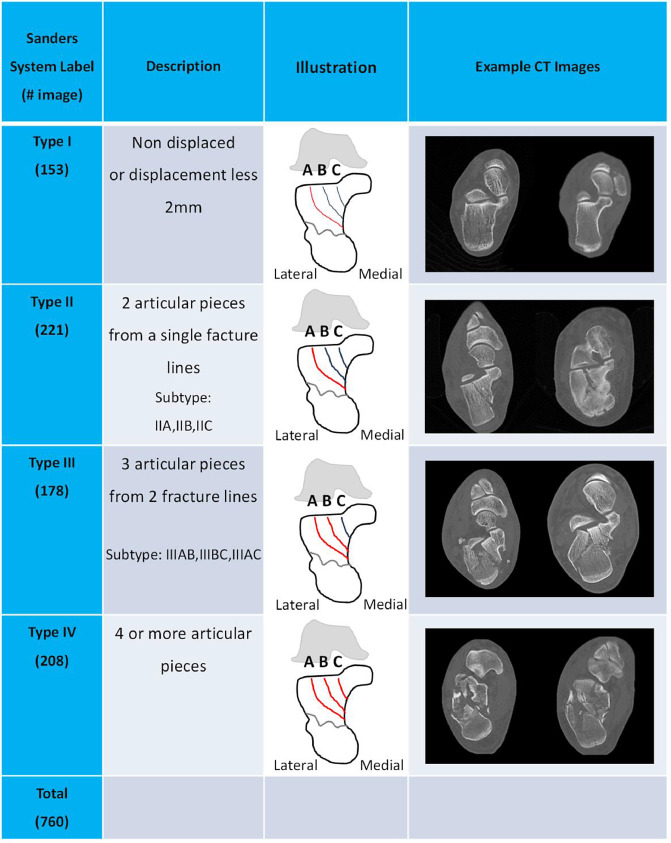
Sanders Classification of Calcaneal Fractures
Midfoot Fractures
Midfoot Sprain Injuries

Navicular Fractures
| Type | Characteristics | Notes |
| Navicular Avulsion | Most common Conservative management | |
| Navicular Tuberosity Fracture | Insertion of the tibialis posterior tendon | ORIF |
| Type I Body Fracture | Transverse in the coronal plane | No angulation of the midfoot |
| Type II Body Fracture | Sagittal with dorsomedial subluxation of the talonavicular joint | |
| Type III Body Fracture | Comminuted fracture with lateral subluxation of the midfoot |
Forefoot Fractures
Lisfranc Injury – low energy trauma
- Lateral or dorsal displacement of M2 on C2 – most reliable
- Step-off sign on lateral view

- >2mm diastasis between M1 and M2 base on AP radiograph
- Fleck sign

Lisfranc Fracture Dislocation – high energy trauma

- Homolateral – all metatarsals displaced laterally
- Divergent – M1 displaced medially, M2-M5 displaced laterally
- Isolated – M1 displaced medially, no other metatarsals displaced
- Don’t get bogged down with all the small fracture fragments
General Forefoot Injuries

- If phalangeal tuft fracture – correlate for nailbed injury to exclude open fracture
- Great toe most common
- Jones fracture – prone to nonunion
- Do not confuse with Os Vesalianum
- Peroneus brevis avulsion – AKA Dancer or Pseudo-Jones Fracture
- March/Stress Fractures – similar
- Freiberg Disease – Osteochondrosis of the metatarsal head
- Adolescents, F>M
- Turf Toe – really a ligamentous injury, sometimes fracture of the sesamoids is called turf toe
- Müeller-Weiss – osteonecrosis of the navicular in adults