Indications
| Indication | Details |
|---|---|
| CSF analysis — infection | Suspected bacterial meningitis, viral meningoencephalitis, fungal CNS infection, Lyme neuroborreliosis |
| CSF analysis — hemorrhage | Suspected subarachnoid hemorrhage with negative head CT (xanthochromia, elevated RBCs) |
| CSF analysis — demyelinating/inflammatory | Multiple sclerosis (oligoclonal bands), neurosarcoidosis, CNS vasculitis, paraneoplastic syndromes |
| Opening pressure measurement | Idiopathic intracranial hypertension (IIH); normal pressure hydrocephalus (NPH) |
| Intrathecal therapy | Chemotherapy (CNS lymphoma, leukemia); antibiotics (fungal meningitis); analgesics |
| CT myelography | Intrathecal contrast injection for CSF leak localization or when MRI is unavailable/contraindicated |
Contraindications
| Type | Contraindication |
|---|---|
| Absolute | Elevated ICP with intracranial mass effect or obstructive hydrocephalus (herniation risk — obtain head CT/MRI first); uncorrected coagulopathy (INR >1.4 or PLT <50,000); overlying skin infection at access site; tethered cord or myelomeningocele at puncture level |
| Relative | Inability to cooperate (sedation may be required); anticoagulation (requires hold — see checklist); pregnancy (fluoroscopy radiation — minimize exposure, consider US-guided); Chiari I malformation (MRI first to assess tonsillar herniation and cisterna magna) |
Always obtain head CT or MRI before LP if there is papilledema, focal neurologic deficit, altered consciousness, or any clinical suspicion for elevated ICP with mass lesion. Performing LP with uncal or tonsillar herniation risk can be fatal.
Relevant Anatomy
Target Interspace
The conus medullaris typically terminates at the L1 vertebral level in adults (range L1–L2). Target the L2–L3 or L3–L4 interspace to remain safely below the conus and in the cauda equina region. The L4–L5 interspace is an acceptable alternative. The iliac crest approximates L4 on the lateral fluoroscopic view.
Tissue Layers Traversed
From superficial to deep (midline approach): skin → subcutaneous fat → supraspinous ligament → interspinous ligament → ligamentum flavum → epidural space → dura mater → arachnoid mater → subarachnoid space (CSF).

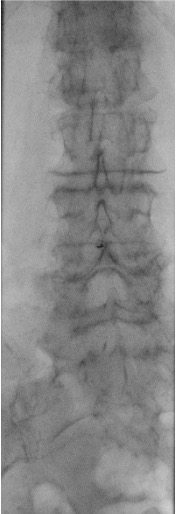
Fluoroscopic Views
When bedside US-guided or blind LP fails, fluoroscopy (prone or lateral decubitus) provides definitive guidance. The PA view confirms midline needle position; the prone oblique view opens the interspace and aligns the X-ray beam parallel to the disc for optimal interlaminar access.


Danger Structures
- Anterior epidural venous plexus: venous blood on aspiration without free-flowing CSF — needle too deep or angled anteriorly; withdraw and redirect
- Cauda equina nerve roots: radicular pain or paresthesias during needle advancement — stop immediately and redirect; do not advance through nerve tissue
- Disc space: avoid direct disc puncture; confirm midline position on fluoroscopy before advancement
Pre-Procedure Checklist
Imaging Review
- Head CT or MRI within 30 days to exclude intracranial mass, obstructive hydrocephalus, or herniation risk
- Lumbar spine MRI or CT review: identify optimal interspace, prior hardware (fusion, instrumentation), severe stenosis, spondylosis, or disc herniation that may alter approach
Labs — SIR Category 2
INR <1.5, platelets >50,000. These thresholds are stricter than Category 1 due to proximity to the spinal cord and risk of spinal hematoma.
Anticoagulation
LP is SIR Category 2 — anticoagulation holds are required. For agent-specific hold times and periprocedural management, use the RadCall IR Anticoagulation Reference →
Patient Positioning
Prone or prone oblique on the fluoroscopy table with a pillow under the abdomen to reduce lumbar lordosis — this opens the interspinous spaces and facilitates needle advancement. Lateral decubitus position is used for opening pressure measurement when needed.
Consent Discussion Points
- Post-LP headache: ~33% (lower with pencil-point needle technique)
- Spinal hematoma: rare but potentially devastating — requires emergent surgical decompression
- Nerve root injury
- Infection/iatrogenic meningitis
- Herniation in patients with elevated ICP (reason to exclude before procedure)
Equipment Overview
- Fluoroscopy unit (C-arm or fixed)
- Sterile drape, prep supplies, and gloves
- Local anesthetic
- Spinal needle: pencil-point (atraumatic) tip preferred over cutting tip to reduce post-LP headache and dural leak
- Manometer and 3-way stopcock for opening pressure measurement
- Four numbered CSF collection tubes
- Extension tubing (for prone positioning)
- Sterile occlusive dressing
Procedure Overview
- Position patient prone with pillow under abdomen; confirm with fluoroscopy that lumbar lordosis is reduced
- Fluoroscopic survey: identify target interspace (L2–L3 or L3–L4), confirm midline, assess interspace width
- Sterile prep and drape; infiltrate local anesthetic from skin down toward the interspace
- Local anesthetic is infiltrated into superficial and deep soft tissues only — do NOT inject into the thecal sac
- Advance spinal needle under fluoroscopic guidance: midline approach for straightforward cases; oblique or paramedian approach for significant degenerative disease or prior fusion
- Confirm subarachnoid position by free-flowing CSF; measure opening pressure with manometer and 3-way stopcock
- Collect CSF into 4 sequential numbered tubes (tube 1: cell count; tube 2: protein/glucose; tube 3: Gram stain/culture; tube 4: cell count — to compare with tube 1 for traumatic tap)
- Replace stylet before withdrawing needle — reduces post-LP headache
- Apply sterile occlusive dressing
Complications
| Complication | Rate | Recognition & Management |
|---|---|---|
| Post-LP headache | ~33% | Positional: worse upright, better supine. Caused by CSF leak through dural defect — NOT volume-dependent. First-line: oral or IV caffeine, aggressive hydration, recumbent rest. Persistent >4 days → epidural blood patch (~90% effective). |
| Spinal hematoma | Rare but devastating | Progressive neurologic deficit (leg weakness, bowel/bladder dysfunction) after procedure. Emergent MRI spine for diagnosis. Neurosurgical consultation for decompression — must occur within 12 h for optimal neurologic recovery. |
| Nerve root injury | Uncommon | Transient radicular pain or paresthesias from needle contact with cauda equina root. Persistent deficits are exceedingly rare. Stop and redirect needle if radicular symptoms occur. |
| Vasovagal reaction | Variable | Especially with prone positioning. Monitor vital signs; IV fluids; supine positioning if occurs. |
| Delayed epidermoid tumor | Very rare | From skin fragment inclusion if needle advanced without stylet. Always use stylet on initial needle insertion — never advance without stylet in place. |
| Iatrogenic meningitis | Rare with sterile technique | Fever and meningismus within 24–48 h post-procedure. CSF Gram stain and culture; antibiotics per culture results. |
Post-Procedure Care
- Recumbent for 30 minutes post-procedure
- Neurologic checks: motor and sensory function of lower extremities before discharge
- Document: opening pressure, closing pressure, CSF appearance, volume collected
- Restrict strenuous activity for 24 hours
- Post-LP headache management: caffeine (oral or IV), aggressive hydration, recumbent positioning; epidural blood patch if headache persists beyond 4 days
CSF Analysis Reference
| Test | Normal | Abnormal / Clinical Significance |
|---|---|---|
| Opening pressure | 7–20 cmH₂O (lateral decubitus) | >25 cmH₂O suggests IIH; >40 cmH₂O strongly elevated; low pressure (<6) suggests CSF leak |
| Appearance | Clear, colorless | Cloudy = infection; bloody = hemorrhage or traumatic tap; xanthochromic (yellow) = SAH or elevated protein |
| WBC | 0–5 cells/μL (lymphocytes) | Elevated neutrophils = bacterial meningitis; lymphocytes = viral/fungal/TB; >10 cells typical for infection |
| RBC | 0 | Elevated in SAH (does not clear tube to tube); traumatic tap clears from tube 1 to tube 4 |
| Protein | 15–45 mg/dL | Elevated in infection, GBS, MS, malignancy, hemorrhage |
| Glucose | 50–80 mg/dL (60–70% of serum) | Low (<45 mg/dL or <60% serum) in bacterial/fungal meningitis; normal in viral |
| Gram stain / culture | Negative | Positive in bacterial meningitis; sensitivity ~80% |
| Cytology | Negative | Positive in leptomeningeal carcinomatosis or CNS lymphoma |
| Oligoclonal bands | Absent (or <2 bands) | ≥2 bands present in CSF only (not serum) supports MS diagnosis |
| Xanthochromia | Absent | Yellow discoloration from oxyhemoglobin/bilirubin; confirms SAH vs. traumatic tap; develops 2–4 h after hemorrhage, persists up to 2 weeks |
When to Escalate
- Progressive neurologic deficit after LP: emergent MRI spine for spinal hematoma; neurosurgical consultation — decompression must occur within 12 h for neurologic recovery
- Headache changing character or non-positional: rule out intracranial hypotension with subdural hematoma on MRI brain
- Fever with meningismus post-LP: meningitis workup — repeat CSF sampling; broad-spectrum antibiotics while awaiting culture results