Lumbar epidural steroid injection delivers corticosteroid and anesthetic into the epidural space to reduce neurogenic inflammation from disc herniation, foraminal stenosis, or facet arthropathy. Image-guided (fluoroscopy or CT) delivery is standard — blind "loss-of-resistance" techniques carry higher false placement rates and procedural risk. The procedure is among the highest-volume image-guided pain interventions performed in radiology, pain medicine, and PM&R practices.
Key points
Three primary approaches: interlaminar (ILESI), transforaminal (TFESI), and caudal. TFESI is the most targeted; ILESI distributes bilaterally; caudal is safest in post-surgical anatomy.
TFESI delivers the steroid closest to the dorsal root ganglion and affected nerve root — highest efficacy for radicular pain from a specific nerve root level, but highest risk of intra-arterial injection and spinal cord infarction (especially at L1–L3 with ascending radiculomedullary arteries).
Non-particulate steroid (dexamethasone) is preferred over particulate (methylprednisolone, triamcinolone) for transforaminal injections — FDA 2014 warning: particulate steroid in an intra-arterial injection can embolize and cause cord infarction/paralysis.
Live contrast (digital subtraction) prior to steroid confirms epidural spread and excludes intravascular, intrathecal, or intraneural placement. This is the single most important safety step.
Fluoroscopic landmarks: AP — pedicles and spinous process midline; oblique — "Scotty dog" with safe triangle inferolateral to pedicle (TFESI); lateral — epidural spread and needle depth confirmation.
Outcomes: 50–75% of patients with disc-related radicular pain experience clinically meaningful relief at 3 months; effect wanes by 6–12 months. Less effective for axial back pain, central stenosis, or failed back syndrome.
Complication rates are low — major adverse events <0.1%; dural puncture 0.5–1%; vasovagal reaction 1–2%; transient numbness common.
Indications and Contraindications
Indication
Notes
Lumbar radiculopathy from disc herniation
Strongest indication; TFESI preferred when single-level nerve root pathology; typically after ≥4–6 weeks of conservative management
Foraminal / lateral recess stenosis
Good candidate for TFESI at the compressed level
Lumbar central canal stenosis (mild-moderate)
ILESI or caudal; evidence mixed but relief often provided for neurogenic claudication
Failed back surgery syndrome (select patients)
Caudal approach often preferred in postsurgical anatomy; more modest outcomes
Post-herpetic radiculopathy
Less common indication; some evidence for TFESI
Diagnostic for level localization
Short-acting anesthetic at a specific level can localize pain generator when clinical and imaging findings are discordant
Type
Contraindication
Absolute
Active systemic infection · Local infection at planned needle entry · Uncorrectable coagulopathy · Allergy to contrast, local anesthetic, or steroid · Pregnancy (fluoroscopy)
Relative
Poorly controlled diabetes (steroid-induced hyperglycemia; counsel and monitor) · Congestive heart failure (fluid/sodium load) · Recent immunosuppression · Active anticoagulation — follow ASRA guidelines for hold timing by agent
Approaches Compared
Approach
Target
Best For
Key Risks
Interlaminar (ILESI)
Posterior epidural space via flavum, midline or paramedian; steroid spreads bilaterally around dural sac
Bilateral symptoms, central pathology, mild-moderate stenosis
Interlaminar lumbar epidural injection — schematic showing needle trajectory through the ligamentum flavum into the posterior epidural space.
Relevant Anatomy
Epidural space: extends from foramen magnum to sacral hiatus; contains fat, vessels (Batson's plexus), and dural sleeves of exiting nerve roots.
Ligamentum flavum: the tissue the needle "pops" through on interlaminar approach; its thickness guides loss-of-resistance technique.
Kambin's triangle / safe triangle (TFESI): bounded superiorly by the pedicle, medially by the dural sac, inferolaterally by the exiting nerve root. The needle tip is placed in the "6 o'clock" position inferolateral to the pedicle on AP.
Radiculomedullary arteries (artery of Adamkiewicz): dominant anterior spinal cord supply; arises from a lumbar or lower thoracic intercostal/lumbar artery (most commonly L1–L2 on the left). Can enter the foramen with the nerve root — inadvertent cannulation during TFESI causes cord infarction.
Sacral hiatus: U-shaped opening at the dorsal sacrum, caudal landmark between the sacral cornua; entry point for caudal injection.
Pre-Procedure Evaluation
Imaging review: recent MRI (or CT myelogram if MRI contraindicated) to confirm pathology, identify target level, and plan approach. Correlate clinical symptoms with imaging findings.
Clinical exam and symptom mapping: dermatomal pain pattern, SLR, reflexes, motor exam — ensure the injection level matches the symptomatic nerve root.
Anticoagulation review (ASRA 2018 guidelines):
ASA/NSAIDs — continue (low-risk procedure)
Clopidogrel — hold 5–7 days
Warfarin — hold 5 days, INR <1.5 (TFESI considered intermediate risk)
DOACs — hold 48–72 hours depending on agent and renal function
LMWH prophylactic — hold 12 h; therapeutic — hold 24 h
Blood glucose counseling for diabetic patients — expect transient hyperglycemia for 3–5 days.
Consent including nerve injury, dural puncture and post-dural puncture headache, rare risk of paralysis (emphasize with TFESI), infection, bleeding, steroid side effects, vasovagal reaction.
Procedure Overview
The following is a high-level summary. Full needle trajectory templates, contrast volumes, injectate recipes by approach, and DSA parameters are available in RadCall Pro.
CT guidance — alternative to fluoroscopy for any of the three approaches. Particularly useful in post-surgical anatomy, obese patients, or when precise needle trajectory is needed to avoid spinal hardware.
Setup
Position: prone with pillow under lower abdomen to reduce lumbar lordosis (improves interlaminar window).
Timeout and site marking: confirm level, side, and approach with imaging-correlated anatomy.
Sterile prep and drape. Continuous pulse oximetry; IV access per protocol.
Local anesthesia: 1% lidocaine skin wheal and deeper infiltration along planned needle track (avoid anesthetizing deep to the target neural foramen on TFESI to preserve paresthesia feedback).
Interlaminar (ILESI) Technique
Identify interlaminar space: AP fluoroscopy; choose L4–L5 or L5–S1 interspace typically. Align spinous process midline.
Needle advancement: 22 G Tuohy or 22 G spinal needle, paramedian approach (avoids interspinous ligament; reduces dural puncture risk). Advance incrementally under intermittent fluoroscopy.
Loss of resistance at ligamentum flavum — saline or air technique (saline is safer — air can cause pneumocephalus in rare dural puncture).
Lateral confirmation: needle tip at posterior epidural line.
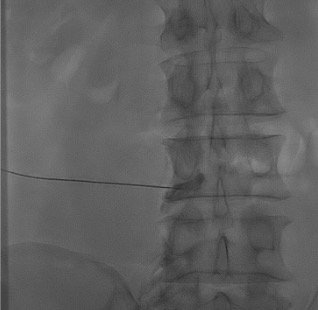
Contrast test dose: 1–2 mL iodinated contrast under live fluoroscopy → expect bilateral epidural spread pattern ("cobweb" or "Christmas tree" shadowing along dural sac and nerve roots).
Inject steroid/anesthetic mixture: e.g., 40–80 mg methylprednisolone or 10 mg dexamethasone in 2–4 mL preservative-free saline + anesthetic.
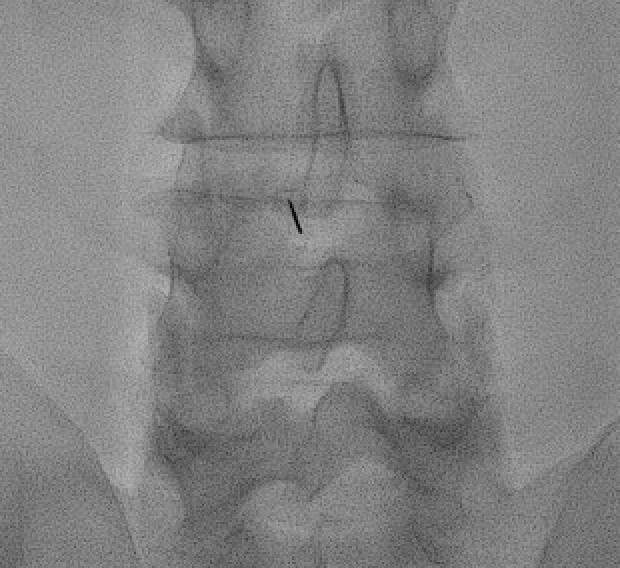
Interlaminar needle placement under fluoroscopy — paramedian approach through the ligamentum flavum at L4–L5 or L5–S1 interspace.Contrast test showing the characteristic epidural spread pattern — tracking bilaterally around the dural sac and along exiting nerve root sleeves. Confirms correct placement prior to steroid injection.
Transforaminal (TFESI) Technique
The "Scotty dog" view on oblique fluoroscopy — pedicle is the eye, transverse process the nose, superior articular process the ear, inferior articular process the foreleg. Needle target is the "6 o'clock" position of the pedicle (eye).
Oblique fluoroscopy to visualize "Scotty dog" at target level — pedicle is the eye; transverse process the nose; superior articular process the ear; inferior articular process the foreleg.
Needle target: "6 o'clock" position of the pedicle (safe triangle) — inferolateral to the pedicle and above the exiting nerve root.
Advance 22 G or 25 G spinal needle toward the target under oblique guidance; rotate to AP and lateral to confirm depth (needle tip at mid-pedicle depth on lateral).
CRITICAL: live digital subtraction angiography (DSA) with contrast test — 1–2 mL iodinated contrast under DSA to identify inadvertent intravascular uptake (rapid washout, linear filling) or intrathecal filling (dural sac fill). Any vascular uptake — reposition and retest.
Epidural confirmation: contrast tracks along the nerve root sleeve and into the anterior epidural space.
Inject non-particulate steroid (dexamethasone 10 mg) + 1–2 mL anesthetic (lidocaine or bupivacaine) slowly.
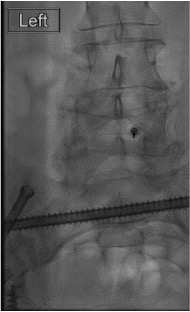
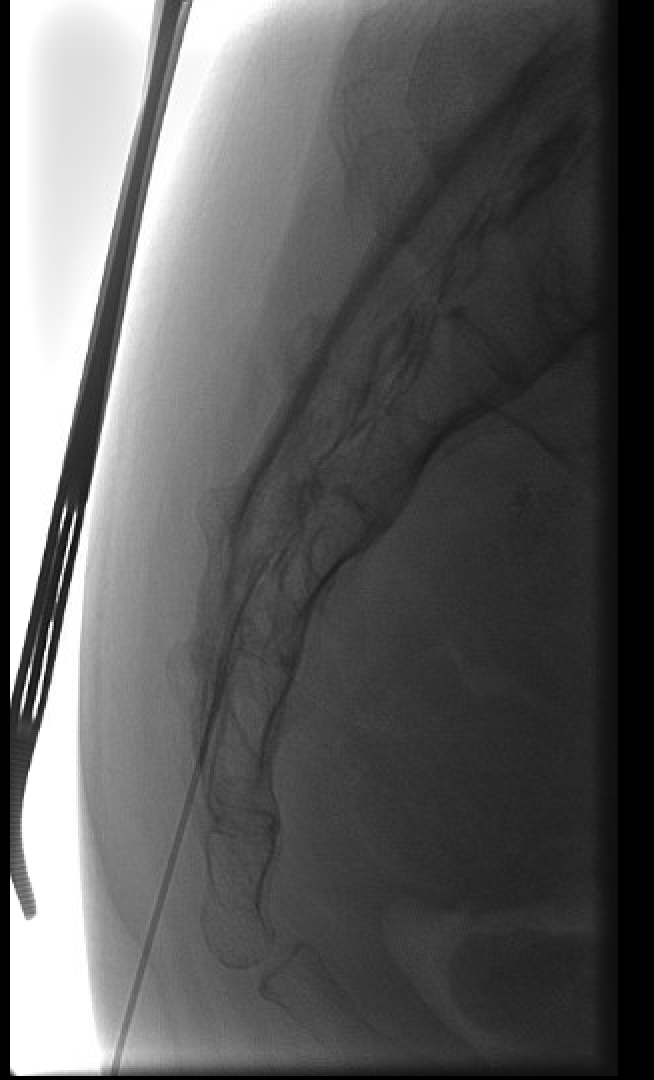
Transforaminal needle positioned at the "6 o'clock" position of the pedicle (safe triangle) — inferolateral to the pedicle and superior to the exiting nerve root.Transforaminal contrast spread along the exiting nerve root sleeve and into the anterior epidural space — confirms epidural placement prior to non-particulate steroid injection.
Caudal Technique
Identify sacral hiatus by palpation (cornua) and lateral fluoroscopy (U-shaped opening at distal sacrum).
Advance 22 G spinal or Tuohy needle through sacrococcygeal ligament at 45° angle, then flatten angle and advance 1–2 cm into sacral canal.
Contrast test: typical "dye in the canal" pattern — ascending epidural spread with sacral nerve root sleeves filling.
Inject larger volume (10–20 mL) of steroid + anesthetic + saline mixture to carry steroid cephalad to the target lumbar level.
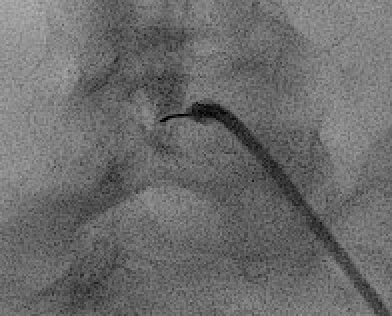
Caudal approach — needle advanced through the sacral hiatus into the sacral epidural canal. Contrast confirms ascending epidural spread.
Injectate Composition
Component
Options and Dose
Corticosteroid — particulate
Methylprednisolone (Depo-Medrol) 40–80 mg; triamcinolone (Kenalog) 40 mg; betamethasone (Celestone) 6–12 mg. Avoid for TFESI due to intra-arterial embolic risk (FDA 2014 warning). Acceptable for ILESI and caudal in most guidelines.
Corticosteroid — non-particulate
Dexamethasone 10–15 mg. Preferred for TFESI. Less commonly used for ILESI/caudal but equally reasonable.
Local anesthetic
Lidocaine 1–2% (fast onset, short duration — good for diagnostic component) or bupivacaine 0.25% (longer duration, potential for motor block at higher concentration). 1–2 mL typical.
Preservative-free saline
Used for volume expansion (ILESI/caudal) or dilution; ensure preservative-free — benzyl alcohol preservatives are neurotoxic.
Contrast
Iodinated low-osmolar (iohexol/Omnipaque, iopamidol/Isovue) 180–300 mg I/mL; 1–3 mL for test dose. Gadolinium is an alternative in iodine allergy but off-label and lower fluoroscopic visibility.
Complications
Complication
Rate
Management
Vasovagal reaction
1–2%
Trendelenburg, IV fluids, atropine if severe bradycardia
Dural puncture / post-dural puncture headache
0.5–1% (ILESI)
Conservative (bed rest, caffeine, hydration); epidural blood patch if persistent >48 h
Transient paresthesia / numbness
Common, self-limited
Reassurance; resolves as anesthetic wears off
Transient exacerbation of radicular pain
5–10%
Self-limited; NSAIDs; reassurance
Transient motor weakness
Rare
From anesthetic spread; observe until resolved before discharge
Intra-arterial injection with spinal cord infarction (TFESI, particulate)
<0.01%
Devastating; prevention via DSA test, non-particulate steroid, and meticulous technique is the only strategy
Infection (epidural abscess, meningitis)
<0.1%
IV antibiotics; neurosurgical drainage if abscess
Epidural hematoma
<0.01%
Emergency MRI and decompression if neurologic symptoms
Limit total annual dose; space injections ≥2 weeks apart; typically ≤3 injections per region per year per consensus
Outcomes
Study / Finding
Result
Radicular pain from disc herniation (short-term, ≤3 months)
Moderate-to-strong evidence for clinically meaningful pain relief; 50–75% of patients experience significant improvement
Radicular pain (long-term, 6–12 months)
Weaker evidence; benefit wanes; may delay or reduce need for surgery in some patients
Central spinal stenosis (neurogenic claudication)
Modest benefit; mixed evidence; generally shorter duration of relief than radiculopathy
TFESI vs ILESI for radiculopathy
TFESI demonstrates greater improvement in pain and function at 2 weeks–3 months in most comparative studies; ILESI remains a reasonable alternative when TFESI is not feasible
Particulate vs non-particulate steroid (TFESI)
Dexamethasone non-inferior to particulate steroids for pain reduction with no risk of embolic cord infarction — preferred per FDA safety review and most pain societies
SPORT trial post-hoc analysis
Patients receiving ESI in addition to surgery or conservative management for lumbar disc herniation: similar long-term outcomes; ESI may facilitate non-operative management
Post-Procedure Care
Observe 15–30 minutes; document neurological exam (ensure no new motor or sensory deficit).
Discharge with instructions: expect 1–3 days of flare (steroid not yet active + needle trauma), then gradual relief over 3–7 days.
Resume normal medications; continue physical therapy and conservative management.
Pain diary if repeat injections planned.
Return for evaluation at 2–4 weeks; repeat injection at 2–4 weeks if initial response was partial (typically ≤3 injections per region per year per consensus).
Diabetic patients: monitor blood glucose closely for 3–5 days.
Evidence Summary
ACR Appropriateness Criteria — Low Back Pain (2021): image-guided epidural steroid injection is appropriate for radiculopathy from disc herniation after ≥4–6 weeks of conservative management.
FDA Safety Communication (2014) — particulate steroids in transforaminal injections: rare but serious neurologic events including spinal cord infarction and paralysis; mandates black-box warning; non-particulate dexamethasone preferred for transforaminal approach.
MSIS / IPSIS / ASRA / SIS Multisociety Pain Workgroup (2015): consensus on safe technique for lumbar TFESI — live DSA or digital spot imaging, non-particulate steroid, and avoidance of sedation that could mask paresthesia feedback.
Cochrane Review (multiple updates): LESI provides short-term pain relief for radiculopathy; evidence for long-term benefit and for axial back pain is less robust.
Manchikanti L et al (Pain Physician ASIPP guidelines): strong evidence for short-term radicular pain relief; moderate evidence for long-term; support for TFESI in single-level radiculopathy.
References
US Food and Drug Administration. FDA Drug Safety Communication: FDA requires label changes to warn of rare but serious neurologic problems after epidural corticosteroid injections for pain. April 2014.
Rathmell JP, Benzon HT, Dreyfuss P, et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology. 2015;122(5):974–984.
Manchikanti L, Knezevic NN, Navani A, et al. Epidural interventions in the management of chronic spinal pain: American Society of Interventional Pain Physicians (ASIPP) comprehensive evidence-based guidelines. Pain Physician. 2021;24(S1):S27–S208.
Bicket MC, Gupta A, Brown CH 4th, Cohen SP. Epidural injections for spinal pain: a systematic review and meta-analysis evaluating the "control" injections in randomized controlled trials. Anesthesiology. 2013;119(4):907–931.
Oliveira CB, Maher CG, Ferreira ML, et al. Epidural corticosteroid injections for sciatica: an abridged Cochrane systematic review and meta-analysis. Spine. 2020;45(21):E1405–E1415.
Mehta P, Syrop I, Singh JR, Kirschner J. Systematic review of the efficacy of particulate versus nonparticulate corticosteroids in epidural injections. PM R. 2017;9(5):502–512.
Kennedy DJ, Zheng PZ, Smuck M, McCormick ZL, Huynh L, Schneider BJ. A minimum of 5-year follow-up after lumbar transforaminal epidural steroid injections in patients with lumbar disc herniation. Spine J. 2018;18(1):29–35.
El-Yahchouchi CA, Plastaras CT, Maus TP, et al. Adverse event rates associated with transforaminal and interlaminar epidural steroid injections: a multi-institutional study. Pain Med. 2016;17(2):239–249.
Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition). Reg Anesth Pain Med. 2018;43(3):263–309.
American College of Radiology. ACR Appropriateness Criteria — Low Back Pain. 2021.
Full technique in RadCall Pro
Complete needle trajectory templates by approach, contrast volume matrices, injectate recipes, DSA parameters, and sedation protocols available in RadCall Pro.