Overview
Type
Location
Classification
Key Points
Femoral Head
Intracapsular
Pipkin (I–IV)
Complication of hip dislocation; I = below fovea; II = above fovea; III + neck fracture; IV + acetabular fracture
Subcapital / Femoral Neck
Intracapsular
Garden (I–IV)
AVN risk increases with grade; I = impacted valgus; II = complete nondisplaced; III = partial displaced; IV = fully displaced. <65 yrs → ORIF; >65 yrs → hemiarthroplasty or THA
Transcervical / Basicervical
Intracapsular
Descriptive
Basicervical = at base of neck, partially extracapsular; less AVN risk; treated like IT fracture
Intertrochanteric
Extracapsular
Evans-Jensen (I–IV)
Stable = intact posteromedial cortex; Unstable = posteromedial comminution, reverse obliquity, or 4-part. Treated with cephalomedullary nail or sliding hip screw
Subtrochanteric
Extracapsular
Descriptive
LT to 5 cm below; high mechanical stress (tension laterally, compression medially); requires cephalomedullary nail. Isolated LT avulsion in adults = malignancy until proven otherwise
Atypical Femoral
Subtrochanteric / shaft
ASBMR Criteria
Bisphosphonate-related; transverse, lateral cortex "beaking," medial spike, minimal comminution, periosteal thickening. Bilateral in 28–47%; image contralateral femur
Hip Dislocation — Reporting Checklist
Direction: posterior (most common, ~90%) vs anteriorPosterior: femoral head displaced superolaterally; lesser trochanter NOT visible on APAnterior: femoral head displaced inferomedially; obturator or ilioinguinal subtypesAssociated femoral neck fracture — closed reduction contraindicated
Associated femoral head impaction fracture (more common anteriorly → THA)
Post-reduction: assess concentricity; femoral head AVN risk (increases with delay >6 hrs)
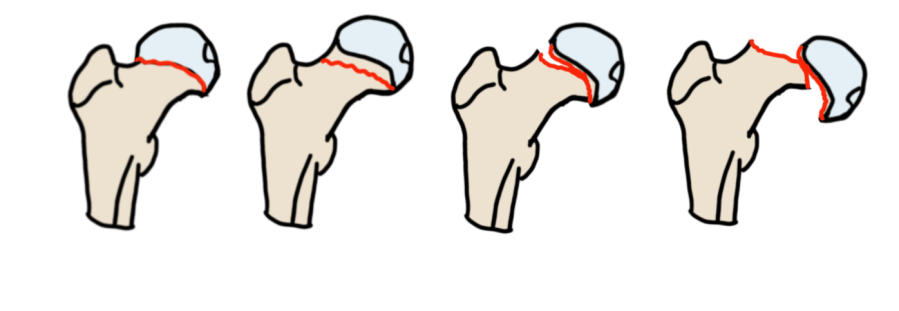
Garden Classification — Femoral Neck
Type
Description
I
Incomplete/valgus impacted — trabecular lines not aligned; head in valgus
II
Complete, nondisplaced — trabecular lines not aligned but no displacement
III
Partial displacement — partial contact between fracture surfaces
IV
Fully displaced — no contact; trabecular lines parallel (realigned by displacement)
Garden classification — femoral neck fractures
Management: <65 yrs → ORIF; >65 yrs → hemiarthroplasty or THA. AVN risk increases with grade.
Femoral Neck Reporting Checklist
Location: subcapital / transcervical / basicervical
Displaced or nondisplaced
Garden grade (higher grade = higher AVN risk)
Contralateral hip imaging if stress fracture suspected
Pauwels Classification — Fracture Line Angle
Type
Angle
Forces
Stability
I
<30°
Predominantly compressive
Stable — favorable for healing
II
30–50°
Mixed compression + shear
Intermediate
III
>50°
Predominantly shear
Unstable — high nonunion/AVN risk
Higher angle = greater shear force = increased instability and AVN risk. More predictive in younger adults.
AVN Risk
Fracture line extending through the lateral femoral head-neck junction (site of lateral epiphyseal vessel entry) carries highest AVN risk.
By location: Subcapital > transcervical > basicervicalBy displacement: Displaced > nondisplacedPosteromedial comminution and lateral head-neck extension on CT are key predictors
Femoral Neck Stress Fractures
Type
Location
Population
Management
Compression
Inferomedial neck (compression side)
Younger athletes; fatigue fracture
Conservative if nondisplaced — tends to self-reduce
Tension
Superolateral neck (tension side)
Elderly; insufficiency fracture
Surgical fixation — high risk of displacement and AVN
Pipkin Classification — Femoral Head (from hip dislocation)
Type
Description
I
Fragment inferior to fovea capitis
II
Fragment superior to fovea capitis (involves weight-bearing surface)
III
Type I or II + femoral neck fracture
IV
Type I or II + acetabular fracture
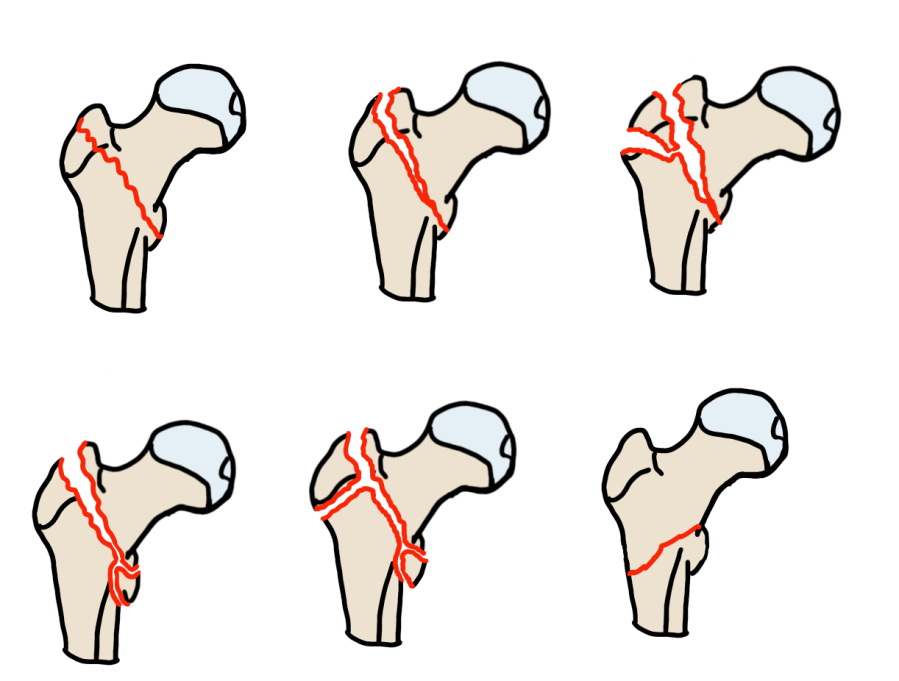
Evans Classification — Intertrochanteric
Key factor = stability, determined by posteromedial cortex integrity .
Type
Pattern
Stability
I
2-part, nondisplaced; fracture line along intertrochanteric line
Stable
II
2-part, displaced; posteromedial cortex intact
Stable
III
3-part; posteromedial cortex comminuted; greater trochanter fragment
Unstable
IV
4-part; posteromedial + greater trochanter + subtrochanteric extension
Highly unstable
Reverse
Fracture line from inferomedial to superolateral; medial displacement of shaft
Highly unstable — nail, not SHS
Evans classification — intertrochanteric fractures
Intertrochanteric Reporting Checklist
Posteromedial cortex: intact (stable) vs comminuted (unstable)
Greater trochanter: separate fragment?
Reverse obliquity pattern (unstable — requires nail, not SHS)
Subtrochanteric extension
Subtrochanteric Fractures
Subtrochanteric zone = lesser trochanter to 5 cm below
High-stress region: lateral cortex under tension, medial cortex under compression → requires cephalomedullary nail
Isolated lesser trochanter avulsion in adults → malignancy until proven otherwise
Russell-Taylor Classification — Subtrochanteric
Type
Piriformis Fossa
Lesser Trochanter
Implication
1A
Spared
Intact
Standard cephalomedullary nail
1B
Spared
Separate fragment
Nail; assess posteromedial cortex
2A
Involved
Intact
Reconstruction nail required (piriformis entry compromised)
2B
Involved
Separate fragment
Most complex; reconstruction nail; greatest instability
Atypical Femoral Fractures — Traumatic vs Atypical
Feature
Traumatic (High-Energy)
Atypical (Bisphosphonate)
Patient
Young, high-energy mechanism
Older; long-term bisphosphonate use (>3–5 yrs)
Fracture orientation
Comminuted, spiral, oblique
Transverse or short oblique
Lateral cortex
Variable
Periosteal thickening / "beaking" or flare
Medial spike
May be present
Characteristic medial spike
Comminution
Common
Absent or minimal
Prodrome
None
Thigh/groin pain before fracture
Bilateral
Rare
28–47% — image contralateral femur
Treatment
Cephalomedullary nail
Cephalomedullary nail; stop bisphosphonate
ASBMR criteria — key imaging features: transverse orientation, lateral cortex periosteal thickening or beaking, medial spike, minimal comminution. Bilateral in 28–47%; always image the contralateral femur.
Reference
Sheehan SE et al. Proximal Femoral Fractures: What the Orthopedic Surgeon Wants to Know. RadioGraphics . 2015;35(5):1563–84.
More in RadCall
99+ guides, IR procedure playbooks, systematic search patterns, case logging, and wRVU tracking — all in one place.
Start free trial ›