Stable Pelvic Fractures
The following fracture patterns are generally considered stable and do not disrupt the pelvic ring:
- Isolated pubic ramus or ischium
- Unilateral both rami
- Isolated sacral fracture (transverse)
- Avulsion fractures
- Duverney fracture (iliac wing; associated with ileus)
Young-Burgess Classification
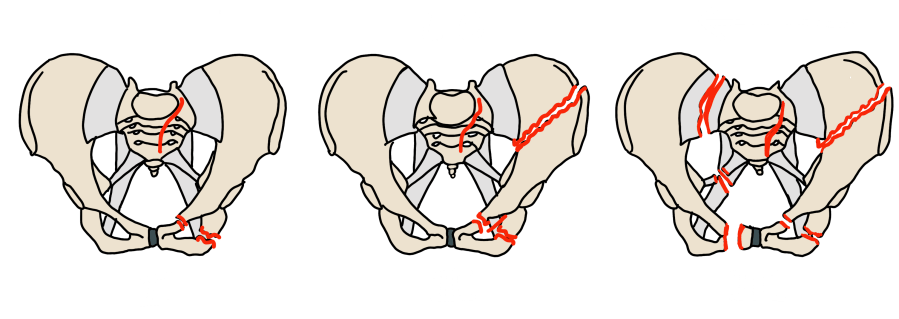
Lateral Compression (LC) — Internal Rotation Force
| Subtype | Fracture Pattern | Stability | Vascular Risk |
|---|---|---|---|
| LC I | Sacral compression fracture (horizontal); ipsilateral pubic rami fractures (usually oblique/horizontal) | Stable; posterior arch intact | Low |
| LC II | LC I + ipsilateral iliac wing fracture ("crescent fracture") — posterior ilium fractures through SI joint, creating a rotational instability | Rotationally unstable; one-sided | Moderate |
| LC III | LC II + contralateral APC injury ("windswept pelvis") — one hemipelvis internally rotated, opposite externally rotated | Highly unstable; bilateral involvement | High — internal iliac on both sides |
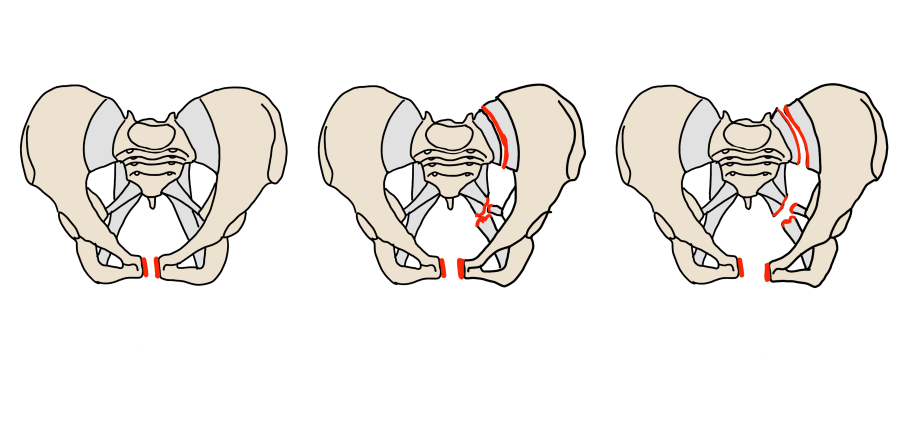
Anteroposterior Compression (APC) — External Rotation Force ("Open Book")
| Subtype | Fracture Pattern | Stability | Vascular Risk |
|---|---|---|---|
| APC I | Symphysis diastasis <2.5 cm; anterior SI joint ligaments intact or minimally disrupted; pubic rami may be fractured anteriorly | Stable | Low |
| APC II | Symphysis diastasis >2.5 cm; anterior SI joint ligament disruption; posterior SI ligaments intact; "open book" with widened anterior SI joint | Rotationally unstable; posterior ring partially intact | High — anterior branches of internal iliac |
| APC III | Complete disruption of all SI ligaments; symphysis diastasis; hemipelvis completely unstable (anterior + posterior ring both disrupted) | Completely unstable | Very high — internal iliac artery injury common; significant hemorrhage; IR embolization often required |
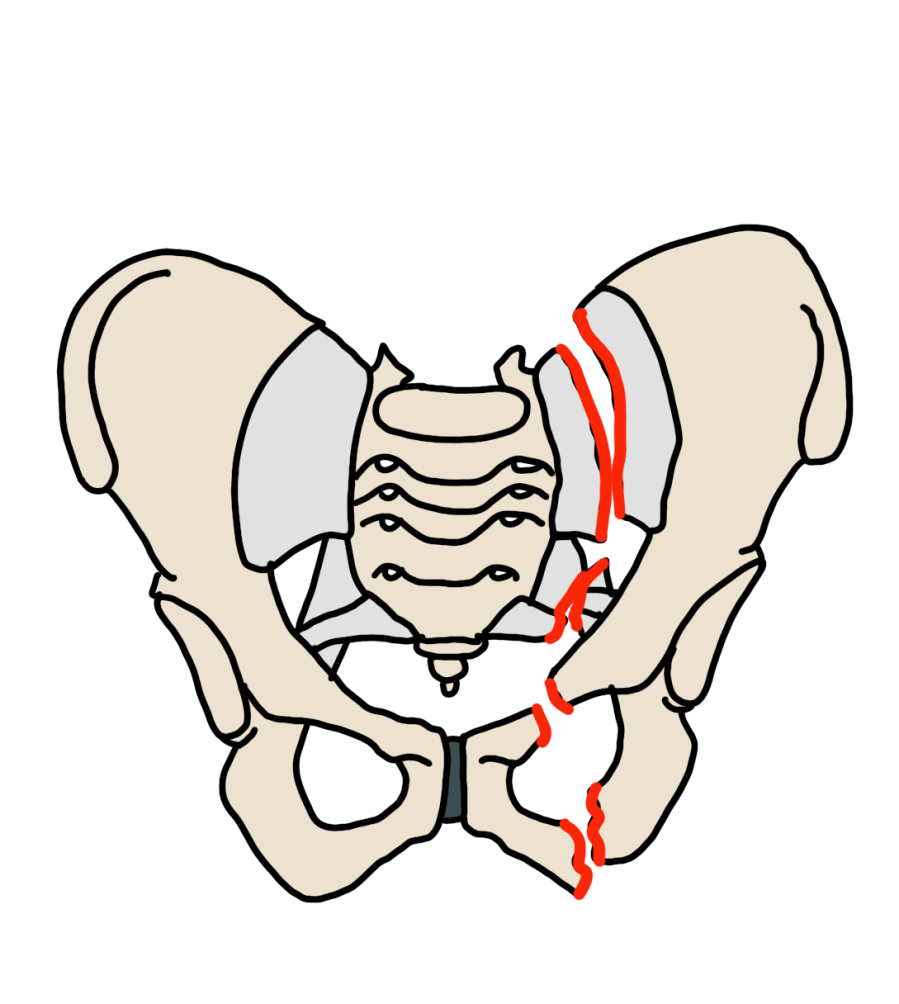
Vertical Shear (VS) and Combined Mechanism (CM)
| Pattern | Description | Stability | Notes |
|---|---|---|---|
| VS | Axial loading with hemipelvis displaced superiorly; disruption of anterior and posterior ring with vertical displacement | Completely unstable | Highest mortality of all patterns; often requires external fixation + embolization; L5 transverse process avulsion common |
| CM | Elements of more than one pattern (e.g., LC + VS) | Variable | Report each component |
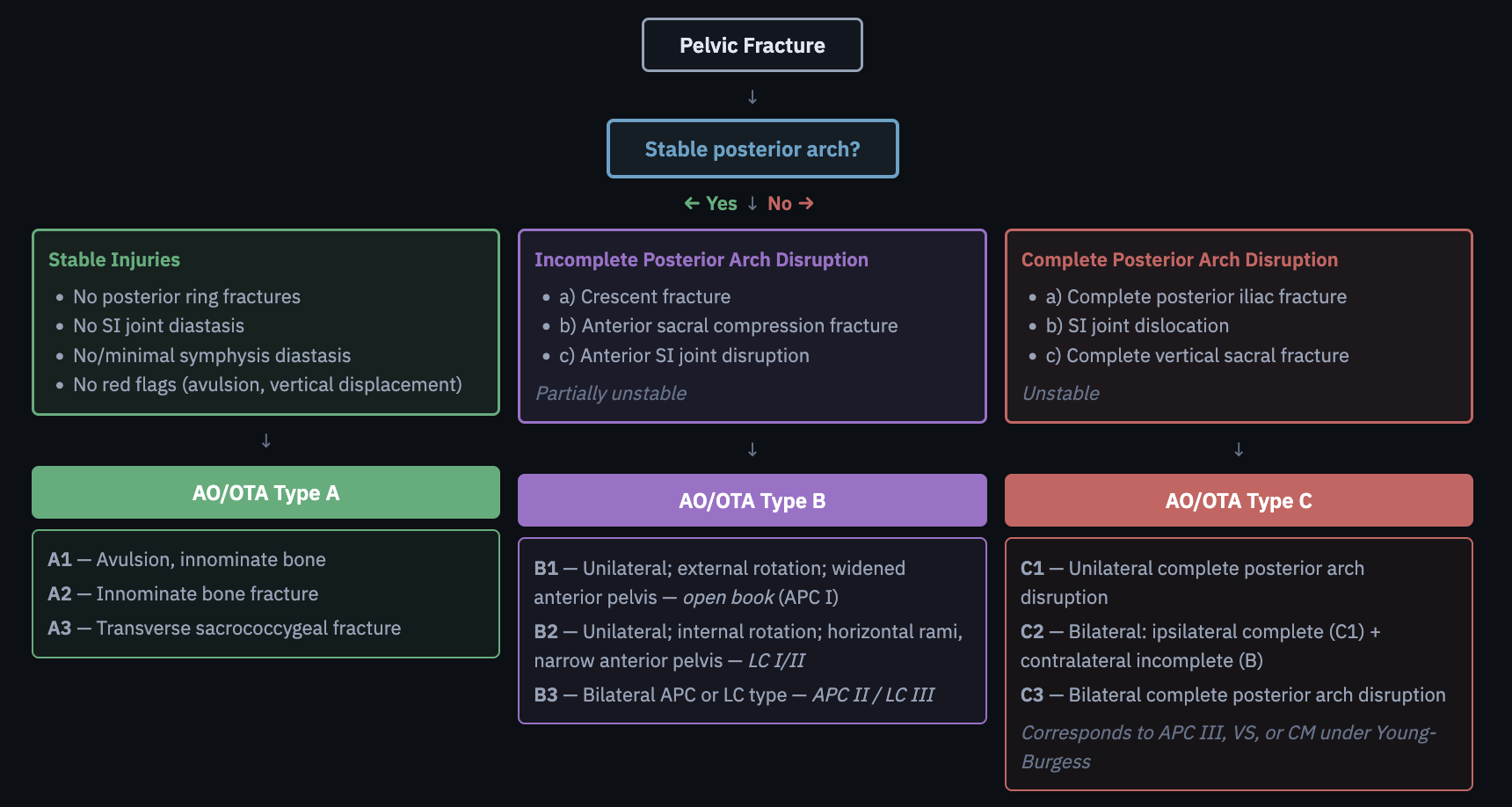
AO/OTA Classification
Type A — Stable
No posterior ring fractures, no SI joint diastasis, no or minimal symphysis diastasis.
| Subtype | Description |
|---|---|
| A1 | Avulsion fracture of the innominate bone |
| A2 | Innominate bone fracture |
| A3 | Transverse sacrococcygeal fracture |
Type B — Partially Unstable (Incomplete Posterior Arch Disruption)
Includes crescent fracture, anterior sacral compression, and anterior SI joint disruption.
| Subtype | Description | Young-Burgess Equivalent |
|---|---|---|
| B1 | Unilateral; external rotation; widened anterior pelvis (open book) | APC I |
| B2 | Unilateral; internal rotation; horizontal rami, narrow anterior pelvis | LC I/II |
| B3 | Bilateral APC or LC type | APC II / LC III |
Type C — Unstable (Complete Posterior Arch Disruption)
Includes complete posterior iliac fracture, SI joint dislocation, and complete vertical sacral fracture.
| Subtype | Description | Young-Burgess Equivalent |
|---|---|---|
| C1 | Unilateral complete posterior arch disruption | — |
| C2 | Bilateral: ipsilateral complete (C1) + contralateral incomplete (B) | — |
| C3 | Bilateral complete posterior arch disruption | APC III, VS, or CM |
Denis Sacral Zone Classification
Sacral fractures are classified by zone of involvement:
- Zone I — Lateral to the sacral foramina; lowest risk of neurologic injury
- Zone II — Through the sacral foramina; risk of unilateral nerve root injury
- Zone III — Central canal involvement; highest risk of bowel, bladder, and sexual dysfunction
Bilateral sacral fractures may form an H-type or U-type pattern and indicate severe instability.
Reporting Checklist
- Classification: AO/OTA Type A (stable) / B (partially unstable) / C (unstable); Young-Burgess: APC / LC / VS / CM — specify grade
- Pubic symphysis: alignment and widening — normal <6 mm in men, <10 mm in women
- Pubic rami: superior and inferior rami; obturator ring — step defect; ipsilateral / contralateral / bilateral
- Iliac bone: fracture lines with or without extension into SI joint (crescent fracture)
- SI joint: symmetry and widening — normal 2–4 mm, wider posteriorly than anteriorly; dislocation
- Sacrum: fracture identification — Denis zone I (lateral) / II (foraminal) / III (central); transverse component; bilateral (H-type / U-type); comminution
- Avulsion fractures: L5 transverse process · inferolateral sacrum · ischial spine · ischial tuberosity · rectus abdominis at pubic crest
- Vasculature: active arterial extravasation (blush) — recommend IR; hematoma — pelvic wall / presacral / rectus sheath
- Pelvic organs: bladder and/or urethral injury; Foley catheter position
- Acetabulum: articular involvement — step-off, intraarticular fragments
Reference
Khurana B et al. Pelvic ring fractures. RadioGraphics. 2014;34(5):1317–1333.