Denis Three-Column Concept
Disruption of ≥2 columns indicates mechanical instability:
- Anterior column: Anterior longitudinal ligament (ALL) + anterior half of vertebral body and disc
- Middle column: Posterior half of vertebral body and disc + posterior longitudinal ligament (PLL)
- Posterior column: Posterior elements (pedicles, facets, laminae, spinous processes, PLC)
AO Spine Classification
Three injury types reflecting progressive instability. Neurologic modifier (N0–N4/NX) appended; "+" added if continued spinal cord compression.
Modifiers:
- M1 = indeterminate tension band injury (may determine need for surgery)
- M2 = patient-specific comorbidity affecting surgical decision (e.g., ankylosing spondylitis, burns)
Type A — Compression
| Subtype | Description |
|---|---|
| A0 | Minor, nonstructural — transverse process or spinous process fracture; no vertebral body involvement |
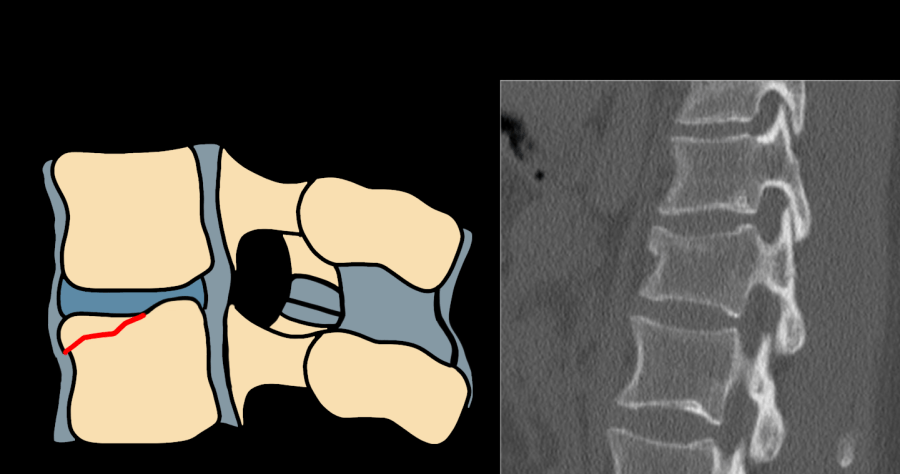
| A1 | Wedge-compression — single endplate; posterior wall intact |
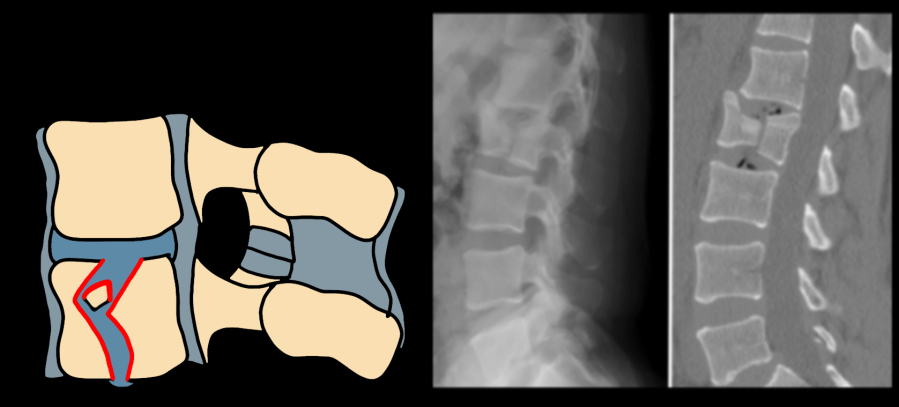
| A2 | Split / pincer — both endplates; posterior wall intact |
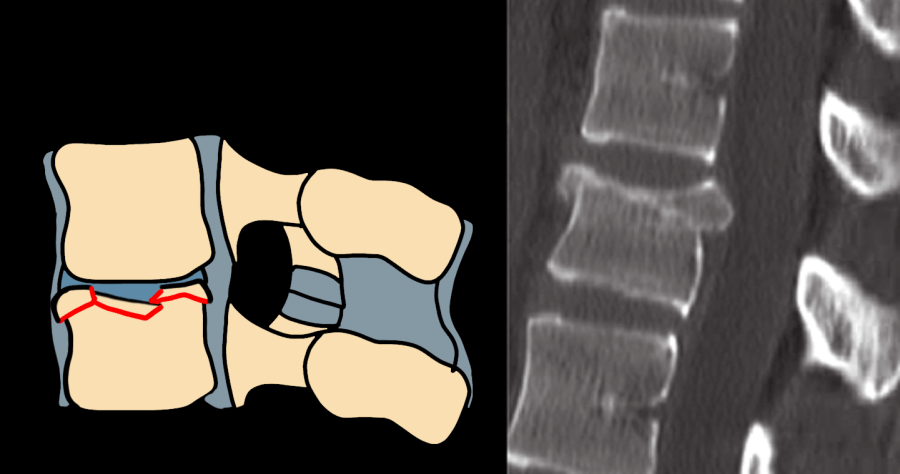
| A3 | Incomplete burst — one endplate + posterior wall involvement; retropulsion present |
| A4 | Complete burst — both endplates + posterior wall; highest compression severity |
Type B — Distraction
| Subtype | Description |
|---|---|
| B1 | Transosseous tension band disruption — monosegmental, pure bony; Chance fracture equivalent |
| B2 | Posterior tension band disruption — osseoligamentous; posterior soft tissue + bone involvement |
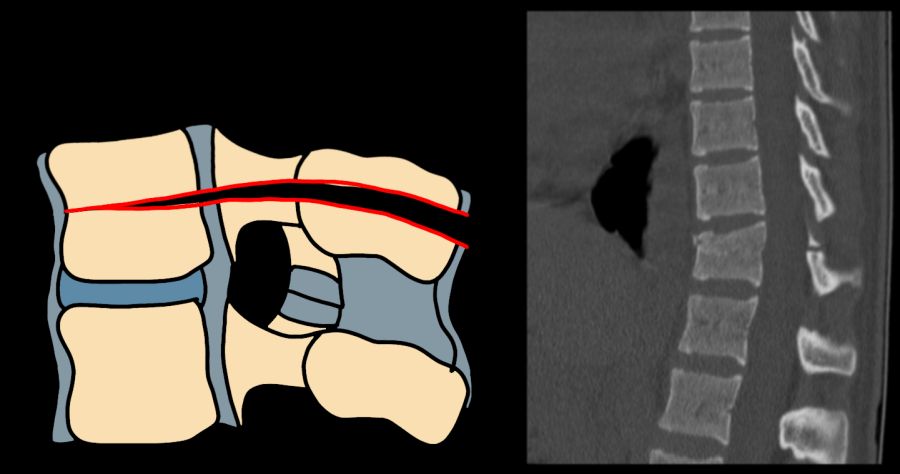
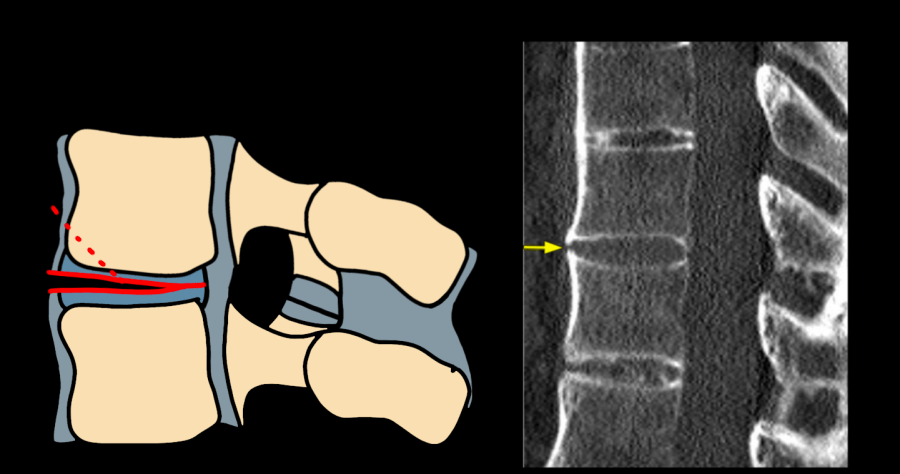
| B3 | Hyperextension — anterior tension band disruption through disc; anterior column distraction |
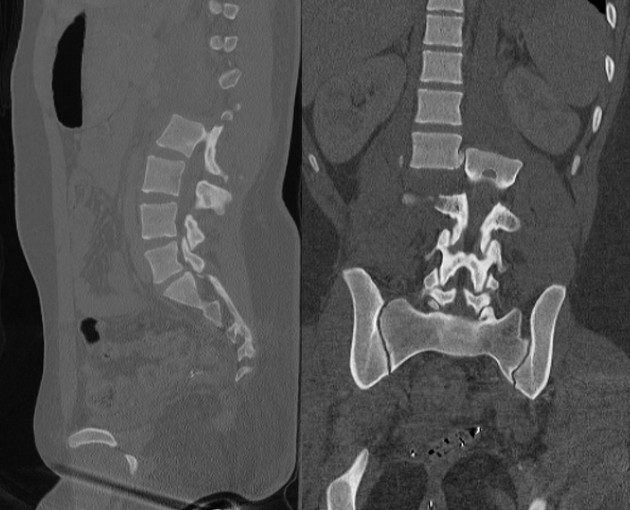
Type C — Translation / Dislocation
| Subtype | Description |
|---|---|
| C | Displacement or dislocation in any plane; complete column disruption; always surgical |
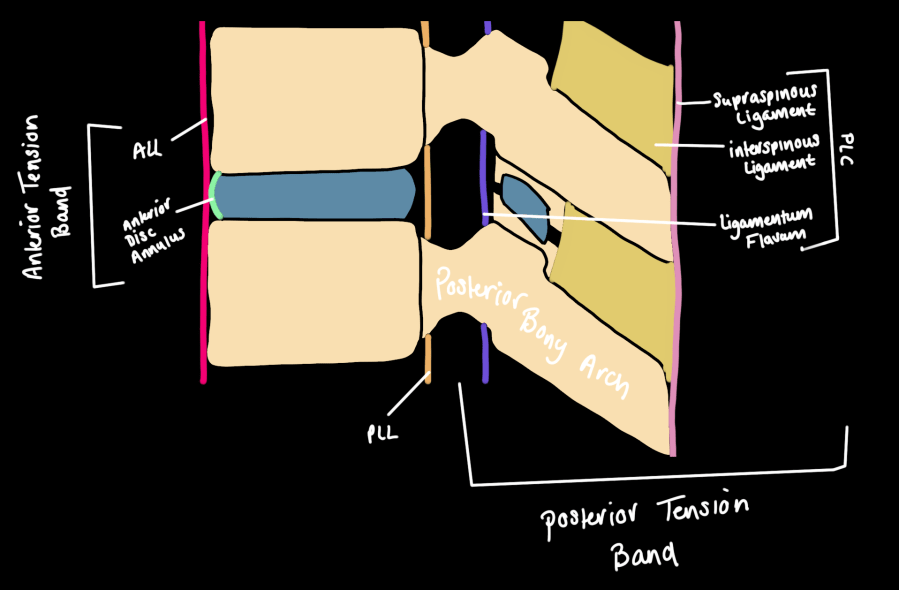
Posterior Ligamentous Complex (PLC)
The PLC = supraspinous ligament + interspinous ligaments + facet capsules + ligamentum flavum. It serves as the posterior tension band — disruption leads to instability, kyphotic progression, and collapse. Poor healing potential usually requires surgical stabilization.
CT signs of PLC disruption (indirect):
- Interspinous distance widening (spinous process splaying)
- Facet joint widening
- Empty / "naked" facet joints
- Perched or dislocated facets
- Spinous process avulsion fracture
- Vertebral body subluxation or dislocation
Posterior endplate avulsion fracture should raise suspicion for flexion-distraction + PLC injury even with minimal kyphosis or height loss. MRI is mandatory before conservative management of burst fractures — osseous retropulsion alone does not indicate PLC injury.
MRI — direct PLC assessment:
| PLC Component | Best Sequence | Intact Appearance | Disruption Finding |
|---|---|---|---|
| Supraspinous ligament | Sagittal T1 or T2 | Continuous dark stripe between spinous process tips | Loss of stripe; T2 hyperintensity replacing dark line |
| Ligamentum flavum | Sagittal T1 or T2 | Continuous dark stripe between laminae | Absence, T2 signal, or fluid at expected location |
| Interspinous ligaments | STIR or fat-sat T2 | Thin hypointense band between spinous processes | T2/STIR hyperintensity (edema); fluid gap = disrupted |
| Facet capsules | Axial fat-sat T2 | Thin hypointense capsular rim; no joint fluid | Capsular fluid/edema; capsular disruption |
Reporting Checklist — Thoracolumbar Trauma
- AO Spine type: A0–A4 / B1–B3 / C; degree of comminution
- Vertebral body height loss: estimate % anterior compression relative to adjacent levels
- Retropulsion: distance (mm); % canal compromise = (1 − x/y) × 100 (x = midsagittal canal at injury; y = mean of levels above and below)
- Degree of kyphosis at injury level
- PLC predictors on CT: interspinous widening / facet widening / naked facets / perched or dislocated facets / spinous process avulsion / vertebral subluxation
- Contiguous and noncontiguous injuries: document all levels
- MRI PLC status (intact / indeterminate / disrupted): supraspinous ligament, ligamentum flavum, interspinous ligaments, facet capsules, ALL, PLL, intervertebral disc
- MRI neurologic injuries: cord/conus signal change / cauda equina compression / nerve root injury / epidural hematoma
- Neurologic modifier (N): N0 intact / N1 transient / N2 radiculopathy / N3 incomplete SCI or cauda equina / N4 complete SCI / NX cannot be examined / + continued compression
- Modifiers: M1 indeterminate tension band / M2 patient-specific comorbidity
Reference
Khurana B, Sheehan SE, Sodickson A, Bono CM, Harris MB. Traumatic Thoracolumbar Spine Injuries: What the Spine Surgeon Wants to Know. RadioGraphics. 2013;33(7):2031–2046.