Fracture Classification by Level
Occipital condyle fractures Classified by morphology and ligamentous involvement. Type III (avulsion of alar ligament) carries instability risk.
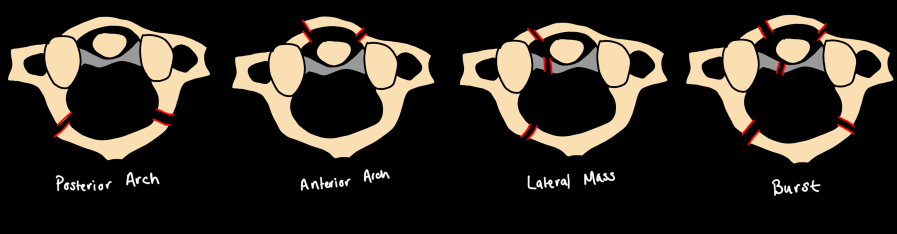
Atlas (C1) — Jefferson Burst Fracture Axial loading causes bilateral fractures through anterior and posterior arches. CT: widening of the atlantodental interval and lateral mass overhang on odontoid view. Transverse atlantal ligament integrity determines stability — MRI required when uncertain.
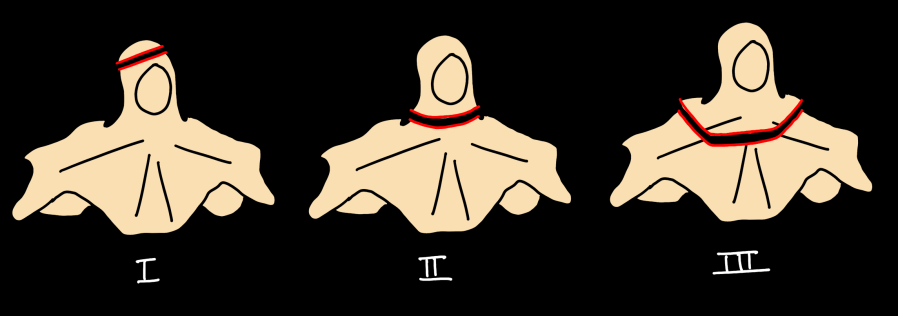
Odontoid Fractures — Anderson-D'Alonzo Classification
| Type | Location | Notes |
|---|---|---|
| I | Tip avulsion | Rare; stable; may indicate atlanto-occipital instability |
| II | Base of odontoid at junction with C2 body | Most common; highest nonunion rate; often requires fixation |
| III | Fracture extends into C2 body | Usually heals with halo immobilization |
Hangman's Fracture — Traumatic Spondylolisthesis of C2 (Levine-Edwards Classification)
| Type | Features |
|---|---|
| I | Bilateral pars fractures, <3 mm displacement, no angulation; stable |
| IA | Atypical — unilateral or asymmetric fracture pattern |
| II | >3 mm displacement OR >11° angulation; disc disruption; unstable |
| IIA | Severe angulation, minimal translation; flexion-distraction mechanism |
| III | Bilateral facet dislocation + pars fractures; most unstable |
Subaxial Cervical Fractures
Hyperflexion injuries:
- Flexion teardrop — anterior-inferior vertebral body avulsion; associated with anterior cord syndrome; highly unstable
- Clay-shoveler's fracture — spinous process avulsion (C6–T1); stable; associated with sudden flexion
- Bilateral facet dislocation — complete ligamentous disruption; >50% anterior subluxation; associated with cord injury
Hyperextension injuries:
- Hyperextension dislocation — posterior element injury with anterior disc disruption; often no fracture on CT; MRI required
- Extension teardrop — anterior-inferior corner avulsion at C2 most common; stable in flexion
Fused spine injuries (DISH / ankylosing spondylitis): High-energy fractures through ossified segments. Typically transverse, through disc space or vertebral body. High cord injury risk. Fractures are often subtle on CT — thin-slice sagittal reformats and low threshold for MRI.
Atlantoaxial rotary fixation (Fielding classification) should be considered in pediatric patients with torticollis after trauma. Dynamic CT in neutral, left, and right rotation is the diagnostic study of choice.