Endovascular repair of thoracic aortic pathology — indications by disease type (BTAI, type B dissection, aneurysm), Ishimaru landing zone anatomy, left subclavian artery management, spinal cord ischemia prevention with CSF drainage, endoleak classification, and surveillance protocol.
Key points
TEVAR has replaced open surgery as the primary treatment for most thoracic aortic pathology — 30-day mortality for TEVAR is 2–5% vs. 10–20% for open repair in comparable lesions.
Adequate proximal seal zone requires ≥20mm of healthy, non-aneurysmal aorta in the intended landing zone — insufficient landing zone may require zone 2 coverage with LSCA management or total arch debranching.
Spinal cord ischemia (SCI) is the most feared complication (2–10%); risk increases with extent of coverage, LSCA coverage, hypotension, and prior aortic surgery; CSF drainage protocol reduces SCI risk.
Left subclavian artery (LSCA) coverage without revascularization is generally tolerated in elective cases when the left vertebral artery is non-dominant and collateral supply is intact; revascularization (carotid-subclavian bypass or transposition) recommended preoperatively for dominant left vertebral, LSCA-dependent left internal mammary CABG, or bilateral arm ischemia risk.
Type B aortic dissection: TEVAR is standard for complicated type B (malperfusion, rupture, rapid expansion) — INSTEAD-XL trial supports TEVAR + medical therapy over medical therapy alone even for uncomplicated type B at 5 years.
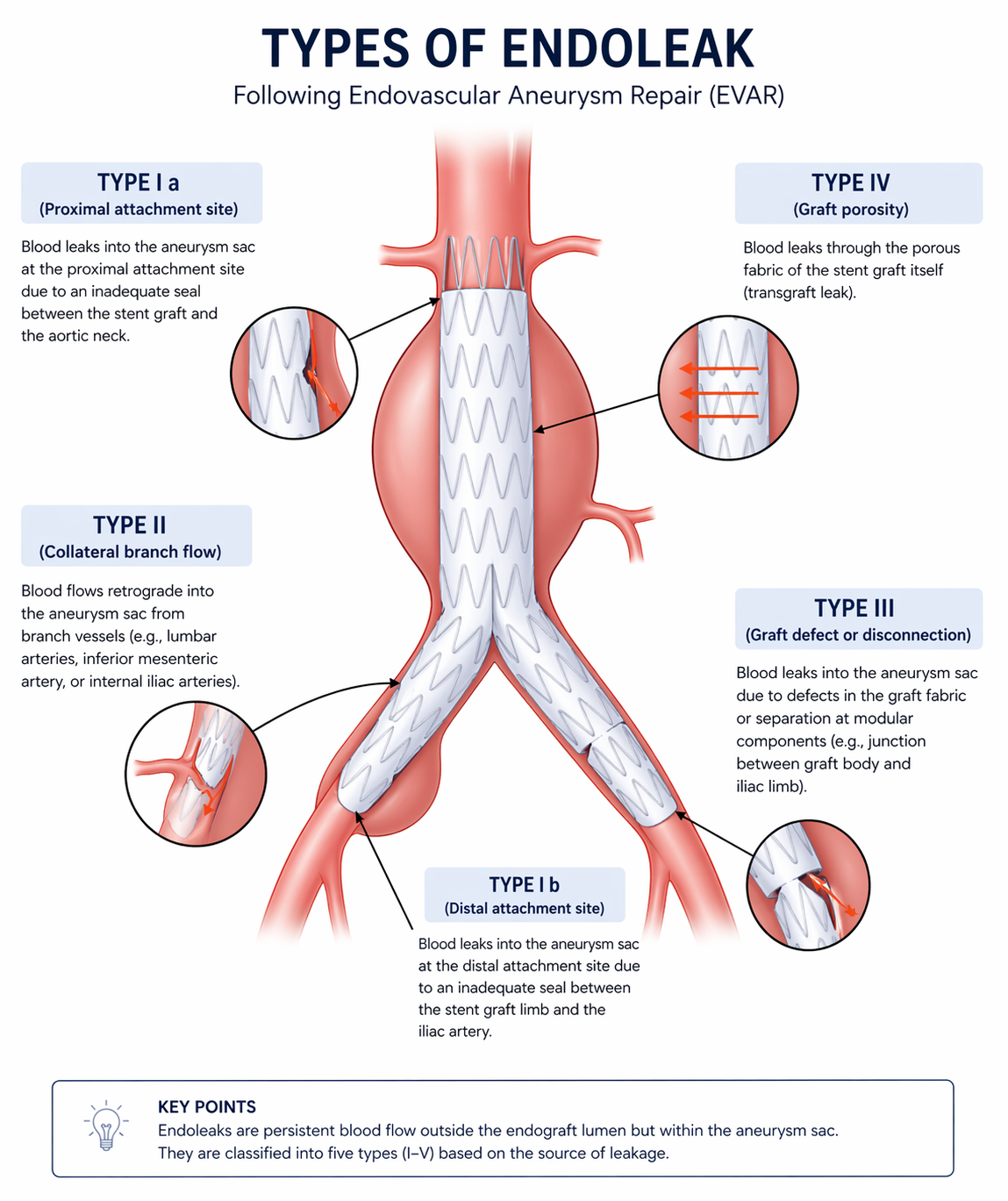
Endoleak types I (attachment site leak) and III (fabric defect/modular disconnect) require urgent reintervention — type II (collateral backflow) and IV (porosity) are usually managed conservatively.
Indications
Indication
Criteria
Urgency
Blunt thoracic aortic injury (BTAI) Grade III–IV
Pseudoaneurysm (grade III) or rupture (grade IV); SVS/AAST classification; TEVAR preferred over open for grades III–IV; grade II (intramural hematoma) — medical management ± delayed repair; grade I (intimal tear) — medical management
INSTEAD-XL trial: TEVAR + optimal medical therapy vs. OMT alone; 5-yr all-cause survival 96.6% vs. 88.9% in TEVAR arm; current guidelines favor TEVAR for uncomplicated type B with anatomic suitability in good surgical candidates
Elective (after medical stabilization)
Thoracic aortic aneurysm (TAA)
Descending thoracic ≥5.5cm (or ≥5.0cm with rapid growth >0.5cm/year, connective tissue disorder, or symptoms); TEVAR preferred over open in patients with adequate landing zones; Crawford/DeBakey extent informs risk
Elective (urgent if symptomatic or rapidly expanding)
Symptomatic or enlarging IMH/PAU; size criteria: PAU ≥20mm depth or ≥10mm penetration; IMH ≥11mm or rapid progression
Urgent if symptomatic; elective if stable with growth
Contraindications
Type
Contraindication
Absolute
Connective tissue disease (Marfan, Loeys-Dietz) — open repair preferred; endograft material is not durable in friable connective tissue; consult vascular/cardiac surgery
Relative
Access vessels too small or tortuous for large-bore delivery system: iliac or femoral diameter <7–8mm (device-dependent); severe tortuosity may require iliac conduit
Relative
Insufficient landing zone (<20mm healthy aorta): requires zone 2 or higher coverage with preoperative arch debranching or hybrid procedure
Relative
Mycotic aneurysm: relative contraindication; endograft infection in contaminated field; open repair or staged treatment preferred in most cases
Absolute
Active aortic infection
Relevant Anatomy
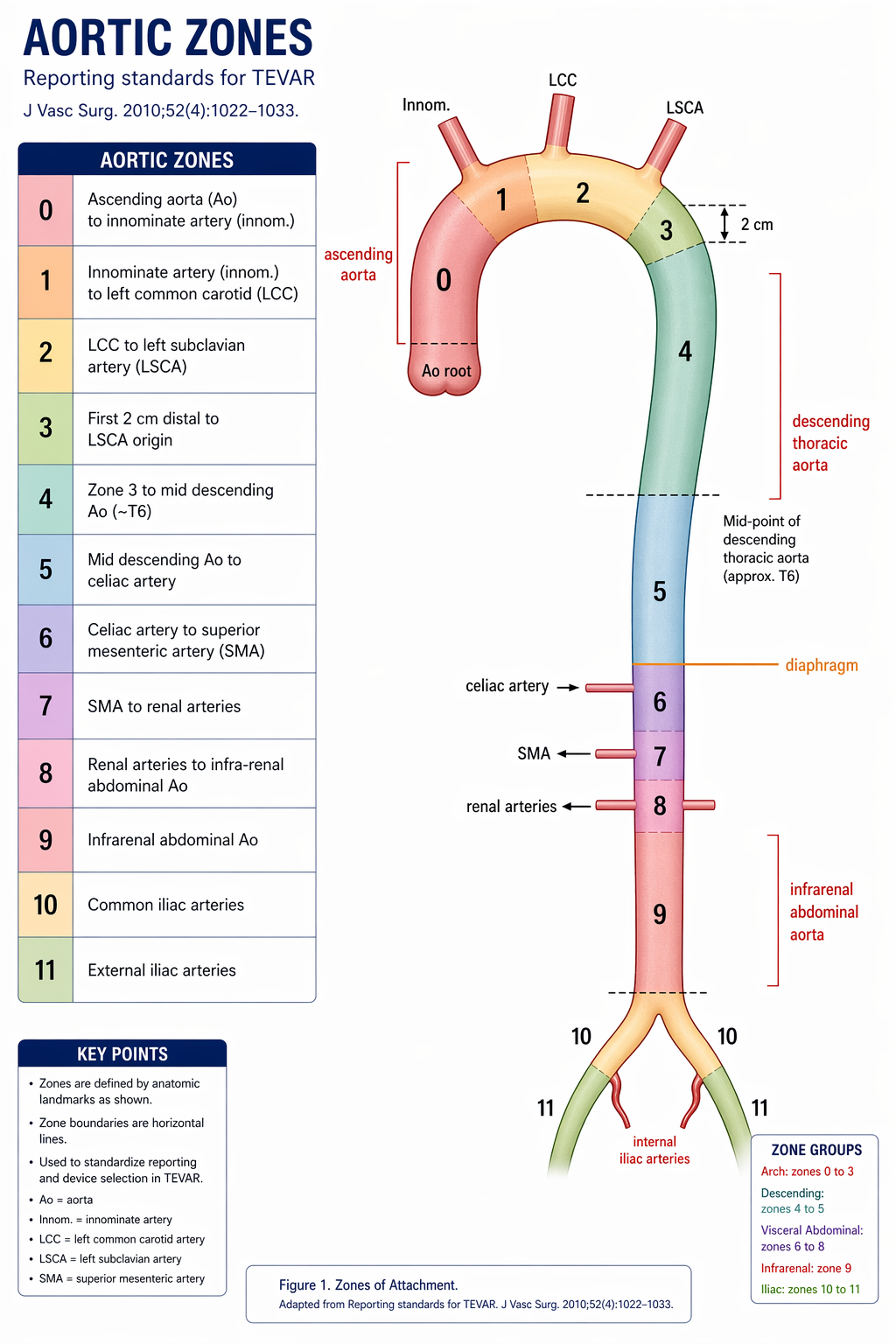
Ishimaru Landing Zone Classification
Zone
Landmark
Notes
Zone 0
Ascending aorta / aortic root
Requires ascending bypass or TAVR hybrid approach
Zone 1
Brachiocephalic / innominate artery origin
Requires innominate and LCCA management; complex hybrid
Zone 2
Left common carotid artery origin
Distal to LCCA — LSCA is covered but LCCA preserved; LSCA management planning required
Zone 3
Left subclavian artery origin
Distal to LSCA — most TEVAR procedures land here or more distally; LSCA preserved
Zone 4
Proximal descending thoracic aorta
Mid-zone 3 to diaphragm; standard landing zone for most TAA and BTAI
Near celiac axis; high SCI risk with extensive proximal coverage
Zones 6–9
Abdominal aorta
EVAR territory; combined TEVAR + EVAR for thoracoabdominal coverage
Most TEVAR for BTAI, type B dissection, and descending TAA lands in zones 2–4. Landing in zone 2 requires LSCA management planning preoperatively.
Aortic landing zones for TEVAR. Zone 2 is the most proximal zone used for standard TEVAR without total arch debranching; zones 0–1 require hybrid arch procedures. Tap to enlarge.
Left Subclavian Artery (LSCA)
Coverage without revascularization: generally tolerated when right vertebral dominant, LSCA not providing LIMA CABG, no prior left carotid occlusion; risk of posterior circulation stroke, left arm claudication (~5%), left arm ischemia (rare)
Artery of Adamkiewicz (greater radicular artery): arises from left T8–L1 in ~75% of patients; primary spinal cord supply in the thoracolumbar region; coverage of this level increases SCI risk substantially
Anterior spinal artery: receives contributions from multiple intercostals plus Adamkiewicz; TEVAR covering long segments eliminates redundancy and collateral reserve
CTA chest/abdomen/pelvis with 3D reconstruction — measure proximal and distal neck diameters, angulation, landing zone length, access vessel diameter and tortuosity, renal artery position relative to intended coverage
Assess for right-dominant vertebral artery on CTA
Confirm ≥20mm of non-aneurysmal, parallel aortic wall in the planned proximal landing zone; assess for thrombus or calcium at landing zone
Multidisciplinary Planning
Cardiac surgery/vascular surgery co-involvement for zone 0–2 cases requiring arch debranching or carotid-subclavian bypass
Anesthesia planning: neuromonitoring (MEP/SSEP), arterial line (right radial for arch cases), large-bore IV access, type and screen; cardiac anesthesia for zone 0–1 cases
CSF drainage catheter: place before or immediately after procedure if planned long coverage (>20cm), LSCA coverage, or prior abdominal aortic surgery
Access Planning
Assess femoral and iliac vessel diameter — device-specific minimum typically 18–24 Fr outer diameter, requiring 6–8mm iliac lumen minimum; measure on CTA with 3D reconstruction
Iliac conduit (8mm Dacron graft to common femoral artery) planned preoperatively by vascular surgery if iliacs are too small or severely calcified
Contralateral femoral access for pigtail marker catheter; brachial artery access for wire snare or arch visualization if needed
Labs and Medical Optimization
CBC, BMP, INR/PT, type and screen (2 units PRBCs available); baseline creatinine (large contrast load anticipated)
Beta-blocker optimization for blood pressure control — target MAP 60–80 mmHg intraoperatively during deployment; hold antihypertensives that cannot be rapidly titrated
Temporary pacemaker wire available for rapid ventricular pacing if precise deployment in difficult arch anatomy anticipated
Consent
Discuss: stroke, spinal cord ischemia/paraplegia, endoleak, device migration, access site complications (hematoma, pseudoaneurysm, iliac injury), conversion to open repair, renal failure from contrast load, LSCA coverage symptoms (arm claudication, posterior stroke), need for secondary interventions, and lifelong CT surveillance requirement.
Procedure Overview
The following is a high-level summary. Full device sizing protocols, landing zone measurement technique, and troubleshooting are available in RadCall Pro.
Access — bilateral femoral arteriotomy or percutaneous (MANTA or Perclose ProGlide pre-closure technique); main device introduced via larger-caliber femoral/iliac; pigtail catheter via contralateral femoral for aortographic marking; if iliac conduit required — vascular surgery creates conduit from 8mm Dacron graft to common femoral artery prior to device introduction
Baseline aortogram — calibrated pigtail at target zone; identify LSCA, LCCA, and renal arteries relative to planned coverage; mark key landmarks with radiopaque ruler or marker catheter; obtain AP and LAO (left anterior oblique) views to profile the arch and landing zone perpendicular to the aortic lumen
Blood pressure management — target MAP 60–80 mmHg during deployment to minimize the "windsock" effect and prevent device migration during release; adenosine-induced cardiac standstill or rapid ventricular pacing (180–200 bpm via temporary pacer wire) used for precise deployment in difficult arch anatomy or high-velocity flow states
Device introduction — advance stiff exchange wire (Lunderquist or equivalent) from access site to ascending aorta; advance delivery system carefully over wire to planned deployment zone; confirm position under fluoroscopy with marker catheter at key landmarks before committing to deployment
Deployment — per manufacturer instructions for use; maintain wire position throughout deployment; deploy proximal seal zone first, then release distally; maintain blood pressure control during deployment; confirm proximal seal zone fully apposed to aortic wall before withdrawing delivery system
Balloon molding — if indicated for incomplete seal or fabric wrinkles at attachment zones; use compliant aortic occlusion balloon sized to aortic diameter; do not over-inflate in the setting of acute dissection (risk of entry tear extension or retrograde dissection)
Completion aortogram — assess for endoleak (type I, II, III); confirm LSCA and arch vessel patency; assess distal perfusion; document length of aortic coverage and landing zones in procedure report; delayed imaging (5 min) if early type I suspected
Access closure — Perclose ProGlide x2 for percutaneous closure at main access site if pre-placed; vascular surgery for cutdown closure if conduit used or percutaneous closure fails; confirm femoral pulse and distal perfusion bilaterally before leaving the suite
Endoleak Classification and Management
Type
Mechanism
Management
Type I (proximal Ia or distal Ib)
Incomplete seal at attachment zones; aortic blood under systemic pressure in excluded sac
Urgent reintervention — balloon molding, proximal or distal extension cuffs, or bare-metal stent in proximal neck to improve apposition; do not observe a type I endoleak
Type II
Retrograde flow from collateral vessels (intercostal arteries, LSCA, celiac) into excluded sac; most common type post-TEVAR
Most resolve spontaneously; observe if sac stable or shrinking; treat if sac enlarging — access via translumbar direct sac injection or catheterization of feeding vessel; coil/glue embolization of feeding collateral
Type III
Fabric tear or modular disconnect between overlapping device components; systemic pressure transmitted to excluded sac
Urgent reintervention — relining with additional endograft component spanning defect; do not observe a type III endoleak
Observe; resolves spontaneously; rarely seen with modern low-porosity devices
Type V (endotension)
Sac growth without identifiable endoleak on standard imaging; occult type I or III most likely
CT with delayed acquisitions (5-minute phase); translumbar direct sac puncture for pressure measurement; treat if confirmed systemic sac pressure or rapidly expanding
Endoleak classification. Types I and III represent failure of seal and require urgent reintervention; type II (collateral backfill) is the most common and is usually observed unless the sac is enlarging. Tap to enlarge.
Spinal Cord Ischemia Prevention
CSF drainage: lumbar drain placed at L2–4; drain when CSF pressure >10 cmH2O (target <10–12 cmH2O); maintain MAP ≥85–90 mmHg post-procedure; drain maintained for 48–72h; limit drainage rate to ≤10–15 mL/h to prevent subdural hematoma from rapid intracranial pressure reduction; clamp and remove when no deficits and adequate time elapsed
Neuromonitoring: MEP/SSEP intraoperative monitoring — signal loss triggers immediate blood pressure elevation and CSF drain placement (if not already in); wake-up test for cooperative endovascular patients in select centers
Blood pressure management: aggressive MAP maintenance (>85–90 mmHg) for minimum 48–72h postoperatively; delayed SCI (up to 5 days post-procedure) occurs in a subset of patients and responds rapidly to blood pressure elevation and CSF drainage if recognized early
Staged repair: for extensive thoracoabdominal coverage (descending thoracic + abdominal aorta), staged TEVAR + EVAR at 4–6 week interval allows time for collateral spinal cord circulation to develop, substantially reducing SCI risk compared to single-stage repair
LSCA revascularization: preoperative carotid-subclavian bypass or transposition reduces SCI risk by preserving the vertebral-anterior spinal artery contribution when LSCA must be covered; perform revascularization before TEVAR in elective cases
Complications
Complication
Rate
Management
Stroke
2–4%
Emboli from wire and device manipulation in aortic arch; minimize by careful wire technique, MAP control, and avoiding unnecessary catheter manipulation in arch; treat per neurology/neurosurgery; tPA contraindicated in early post-TEVAR period due to bleeding risk
Spinal cord ischemia (SCI)
2–10% (higher with extensive coverage)
Immediate MAP elevation to >90 mmHg; CSF drainage if not already placed; high-dose steroids (controversial, limited evidence); neurology consultation; delayed SCI presenting up to 5 days post-procedure responds to blood pressure augmentation if treated promptly
Endoleak
Types I and III: require urgent reintervention; type II: usually observed
See Endoleak Classification section above
Access complications
5–10%
Femoral hematoma, pseudoaneurysm, iliofemoral thrombosis, iliac rupture from large-bore delivery system; covered stent-graft (e.g., Gore Viabahn, iCast) for contained iliac rupture; balloon occlusion for hemorrhage control; vascular surgery for open repair
LSCA ischemia
~5% arm claudication
Left arm claudication (most resolve with collateral development), posterior circulation stroke (rare if revascularized preoperatively), subclavian steal phenomenon; carotid-subclavian bypass for persistent symptomatic arm ischemia
Device migration
1–3% long-term
Detected on follow-up CT imaging; proximal extension cuff for migration away from seal zone; surgical explant for catastrophic migration threatening arch vessels
Retrograde type A dissection
1–2%
Entry tear migrating proximally into ascending aorta; catastrophic complication requiring emergency cardiac surgery (ascending aorta repair, Bentall procedure); TEVAR-caused retrograde type A dissection carries very high mortality; do not attempt endovascular correction
Renal failure
3–8%
Large contrast load, hemodynamic compromise, inadvertent renal artery coverage; pre-hydration with isotonic saline, minimize contrast volume, CO2 angiography supplement in established CKD; avoid NSAIDs and nephrotoxins perioperatively
Post-Procedure Care
ICU admission minimum 24h; continuous arterial line monitoring; MAP target ≥85–90 mmHg for 48–72h for SCI prevention; adjust antihypertensives carefully to maintain MAP above threshold without overshooting
CSF drain management: maintain CSF pressure <10 cmH2O for 48–72h; monitor drain output and neurological deficits every 1–2h; limit drainage rate to ≤10–15 mL/h; clamp drain prior to removal after adequate clinical observation period with no deficits
Daily neurological assessment: new motor or sensory deficit prompts immediate MAP elevation to 90–100 mmHg, CSF drain (if not in place), emergent CT to exclude new endoleak or other causative pathology, and neurology consultation
CT surveillance: CTA at 1 month, 6 months, 12 months, then annually — assess sac size trajectory, endoleak presence and type, device position and integrity, LSCA and arch vessel patency; plain chest radiograph at each annual visit for device fracture detection
Blood pressure control: beta-blocker plus ACE inhibitor for dissection patients; target SBP <120 mmHg chronically to reduce aortic wall stress and limit dissection progression in untreated segments
When to Escalate
Retrograde type A dissection — emergency cardiac surgery (ascending aorta repair/Bentall procedure); extremely high mortality; do not attempt endovascular correction of a TEVAR-caused type A dissection
Type I or III endoleak on completion or follow-up angiogram — reintervention before discharge (type I identified intraoperatively) or urgently on follow-up (type III); do not observe either type under any circumstances
Paraplegia/paraparesis after TEVAR — immediate MAP elevation to 90–100 mmHg; CSF drain placement if not in place; neurology consultation; MRI spine if hemodynamically stable; early intervention within 24–48h dramatically improves neurological outcome
Femoral/iliac rupture during delivery system introduction — covered stent-graft (Gore Viabahn or iCast) for contained rupture; balloon occlusion for temporary hemorrhage control; vascular surgery for open repair; have covered stents available in suite before introducing large-bore delivery systems
Sac expansion on follow-up without identifiable endoleak — delayed-phase CTA with 5-minute acquisitions to identify occult type I or III; translumbar direct sac puncture for pressure measurement; consider endograft relining if systemic sac pressure confirmed or sac rapidly expanding
References
Lee WA et al. Endovascular repair of blunt traumatic thoracic aortic injury: is it ready for widespread adoption? J Vasc Surg. 2013.
Erbel R et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J. 2014;35(41):2873–2926.
Nienaber CA et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection (INSTEAD-XL). Circ Cardiovasc Interv. 2013;6(4):407–416.
Dake MD et al. Endovascular stent-graft placement for the treatment of acute aortic dissection. N Engl J Med. 1999;340(20):1546–1552.
Preventza O et al. Risk factors for spinal cord deficit after endovascular repair of the thoracic aorta. Ann Thorac Surg. 2018.
Society for Vascular Surgery / American Association for Vascular Surgery. Clinical practice guidelines for the management of blunt thoracic aortic injury. J Vasc Surg. 2011.
Full technique in RadCall Pro
Full device sizing protocols, landing zone measurement technique, CSF drainage management, endoleak reintervention strategies, and hybrid arch debranching coordination available in RadCall Pro.