Genicular Artery Embolization (GAE) for Knee Osteoarthritis
Genicular artery embolization is a minimally invasive outpatient procedure that targets pathologic synovial neovascularity in knee osteoarthritis. Chronic inflammation in the osteoarthritic knee drives angiogenesis and sympathetic nerve sprouting — the same abnormal vessels that sustain synovitis also deliver the pain signal. Selective embolization of hypertrophied genicular arteries reduces synovial inflammation and pain in patients with mild-to-moderate knee OA who have failed conservative therapy but are not yet surgical candidates.
Key points
Target population: symptomatic knee OA (Kellgren–Lawrence 1–3) with moderate-to-severe pain, failed ≥3 months conservative management (NSAIDs, PT, intra-articular injections), and not yet a candidate for (or declining) total knee arthroplasty.
Mechanism: chronic synovitis induces pathologic neovascularization and sympathetic nerve co-sprouting; embolization reduces synovial perfusion, angiogenic signaling, and nociceptive input.
Anatomy: five main genicular arteries — descending genicular (from SFA) and four branches from the popliteal artery: superior medial, superior lateral, inferior medial, inferior lateral; plus middle genicular and recurrent branches. All are potential targets.
Target identification: angiographic "blush" or hypervascular synovium corresponding to the zone of maximal pain on physical exam (medial-sided, lateral-sided, or anterior).
Clinical outcomes: GENESIS (Bagla 2020) — WOMAC pain reduction sustained at 24 months; Landers RCT (2023) — superior to sham at 12 months for pain and function in moderate-to-severe OA.
Key complication: cutaneous non-target embolization producing transient skin discoloration or (rarely) skin necrosis; occurs in up to 10–20% with permanent microspheres and is less common with imipenem/cilastatin.
Indications and Patient Selection
Criterion
Detail
Symptom severity
Moderate-to-severe knee pain (VAS ≥4/10 or WOMAC pain subscale elevated) for ≥3 months
Radiographic severity
Kellgren–Lawrence grade 1–3 (GAE is generally less effective for K–L 4 — consider TKA). Some operators include select K–L 4 patients who are poor surgical candidates.
Failed conservative therapy
≥3 months of NSAIDs, physical therapy, activity modification; typically at least one intra-articular injection (corticosteroid and/or hyaluronic acid) that has failed or lost efficacy
Not ready for / declining TKA
Young for TKA (typically <65), medically unfit for TKA, or preferring to avoid/delay surgery
Localized pain
Pain on physical exam localizable to a specific region (medial, lateral, anterior) — correlates with angiographic target selection
Type
Contraindication
Absolute
Active knee infection · Rheumatoid arthritis or other inflammatory arthropathy (GAE not studied; mechanism differs) · Uncorrectable coagulopathy · Severe contrast allergy (if cannot premedicate)
Relative
Severe peripheral arterial disease limiting catheter delivery · Kellgren–Lawrence grade 4 with severe malalignment (limited benefit) · Prior TKA on the target knee · Pregnancy · Vascular access limitations
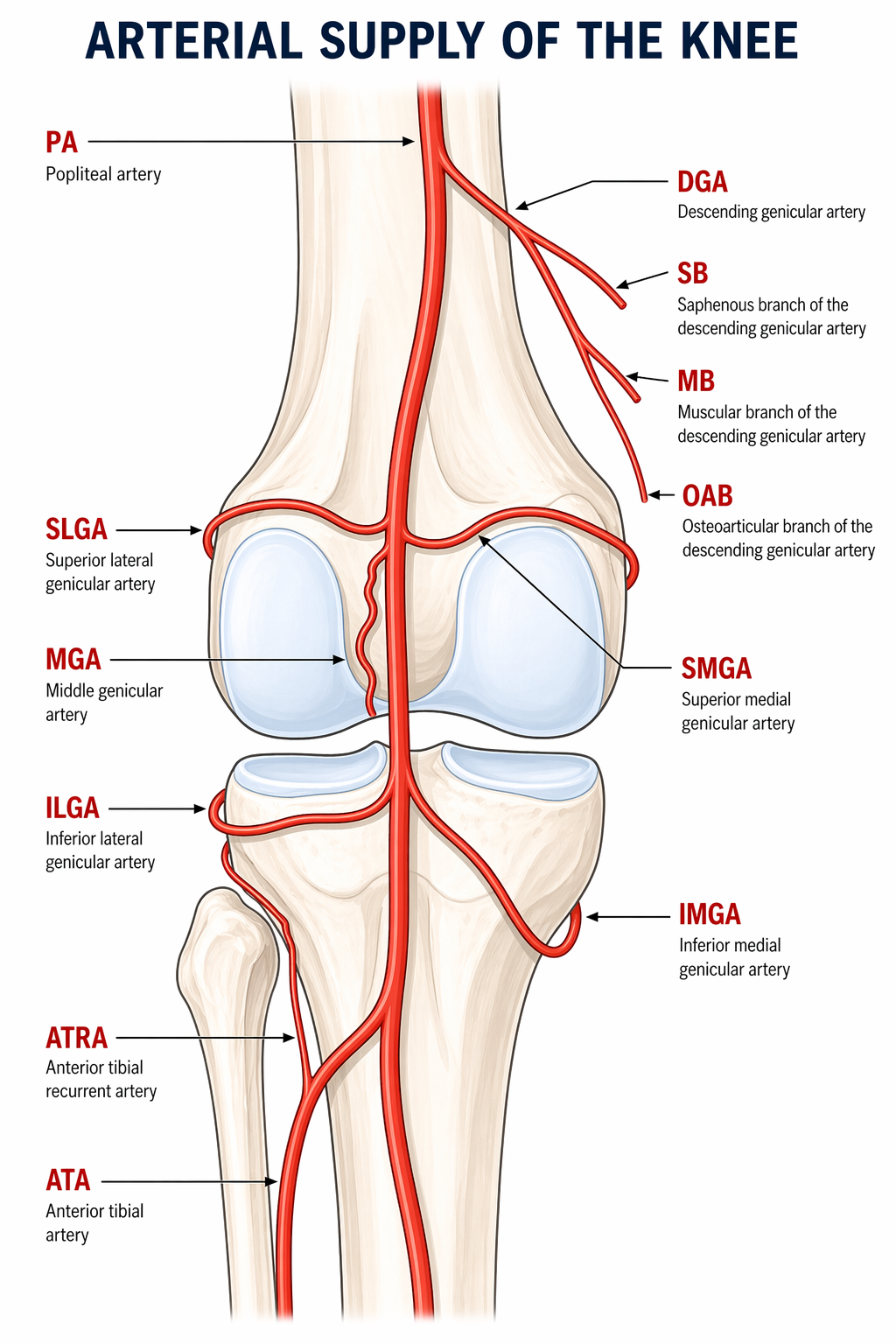
Genicular Artery Anatomy
The knee has a rich periarticular arterial network (the genicular anastomosis) sourced from the superficial femoral artery (SFA), popliteal artery, and anterior tibial artery. The principal targets for GAE are:
Artery
Origin
Territory
Descending genicular (DGA)
Distal SFA, just proximal to adductor hiatus
Anteromedial knee; contributes to medial synovium and capsule
Anterior tibial artery (anterior and posterior tibial recurrent)
Anterior capsule and infrapatellar fat pad
Knowledge of anastomoses is essential — non-target embolization to the saphenous branch of the DGA or cutaneous branches of the SMGA/SLGA is the most common source of complications.
Genicular artery anatomy — descending genicular (DGA) from the SFA and the superior/inferior medial and lateral genicular branches from the popliteal artery, forming the periarticular anastomosis of the knee.
Osteoarthritis is classically considered a "wear and tear" cartilage disease, but the pain phenotype is driven largely by chronic low-grade synovitis. Synovial biopsies in painful OA show:
Hypertrophy and infolding of the synovial lining
Neovascularization (increased vessel density) with immature, fragile vessels
Co-sprouting of unmyelinated nociceptive nerves alongside new vessels (the same angiogenic factors — VEGF, NGF — drive both)
Inflammatory cytokine release (IL-6, TNF-α) sustaining the cycle
Embolization of the abnormal neovascularity reduces synovial perfusion, downregulates inflammatory signaling, and — via pruning of the nerve–vessel pairs — decreases nociceptive input. The rapid onset of pain relief (often within 1–4 weeks) is faster than structural cartilage changes would allow, consistent with this mechanism.
Pre-Procedure Evaluation
Evaluation
Role
Clinical exam
Localize pain (medial, lateral, anterior) — guides angiographic target selection. Document effusion, range of motion, ligamentous stability, and exclude referred pain (hip OA, lumbar radiculopathy).
Weight-bearing knee radiograph
Kellgren–Lawrence grading; exclude severe malalignment; baseline
Knee MRI (optional)
Characterize synovitis (contrast-enhanced if available), meniscal tears, subchondral edema; exclude alternative diagnoses (AVN, tumor, occult fracture)
Pain scoring
Baseline VAS, WOMAC (pain/stiffness/function), KOOS — for outcomes tracking
Vascular review
Assess femoral pulses and peripheral vascular status; review any prior vascular imaging; CTA/duplex if severe PAD suspected
Skin assessment
Document baseline skin color and integrity over the knee — for comparison if post-procedure skin changes occur
Procedure Overview
The following is a high-level summary. Full microcatheter selection, cone-beam CT parameters, and detailed particle sizing algorithms are available in RadCall Pro.
Access and Catheterization
Access: contralateral common femoral artery (6 Fr sheath) is most common; antegrade ipsilateral femoral and radial access are alternatives. Outpatient with moderate sedation.
Baseline angiography: SFA and popliteal artery runs in AP and oblique projections to identify all genicular arteries and their branching patterns.
Selective catheterization: 4 Fr catheter (Cobra, Berenstein, or SOS Omni) to engage the popliteal; 2.0–2.4 Fr microcatheter coaxially advanced into each target genicular artery.
Target Identification
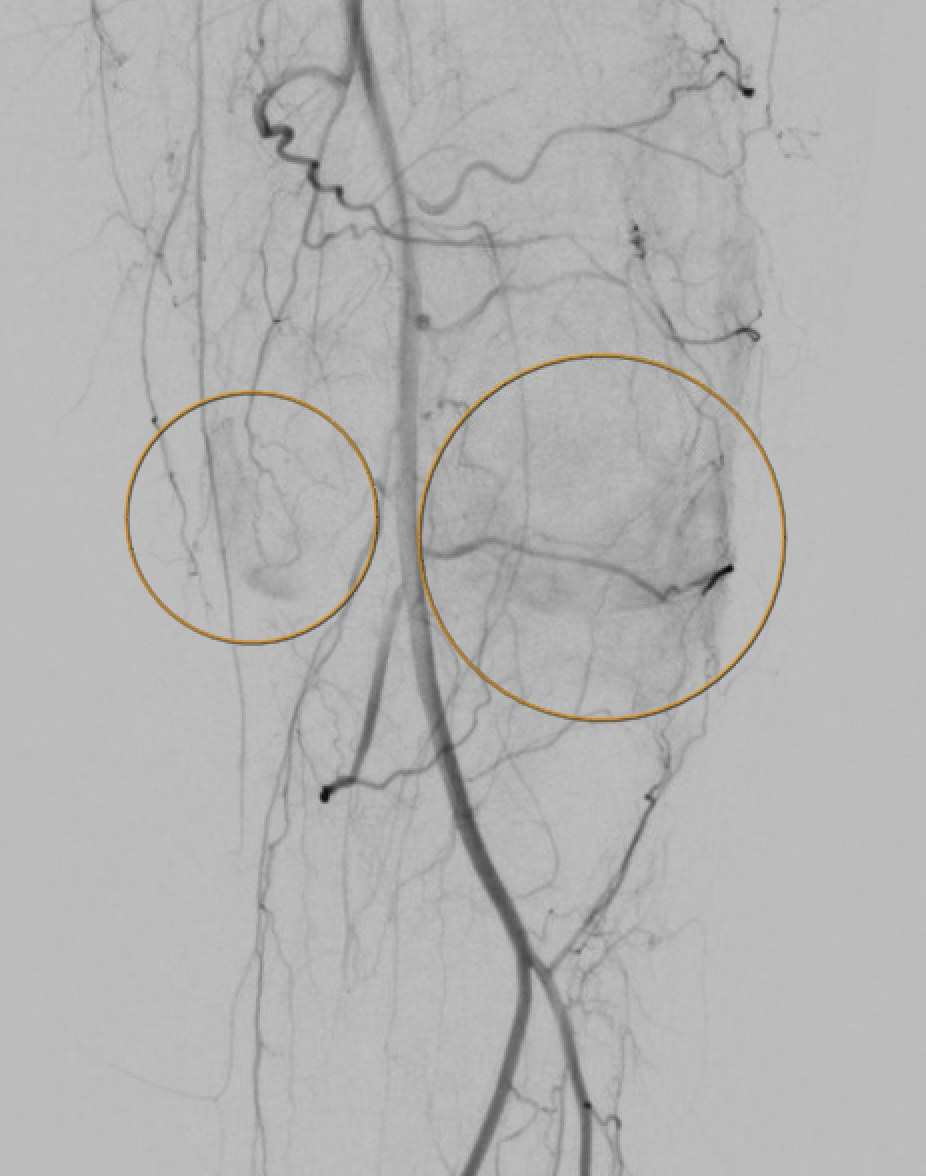
Angiographic hyperemia / synovial blush in the symptomatic territory is the primary target. This appears as a late-phase parenchymal blush beyond the normal capsular stain.
Calibrated microspheres 75–300 μm (Embozene, Embosphere, HydroPearl) — permanent; most common in Western practice.
Imipenem/cilastatin slurry (Okuno technique) — temporary embolic; dissolves within hours to days; favored in Japan and by operators concerned about long-term consequences of permanent particles.
Slow, fluoroscopic injection with 50% contrast dilution; endpoint is near-stasis or pruning of the hyperemic blush while preserving proximal flow to normal tissue.
Reassess after each vessel — completion angiogram to confirm treatment of the blush and exclude non-target deposition.
Skin check during and after the procedure — any skin blanching or patchy discoloration indicates non-target cutaneous embolization; warm compresses and monitoring.
Pre-embolization selective genicular angiogram demonstrating hypertrophied vessels and synovial hypervascularity in the territory of the patient's pain.Post-embolization angiogram showing pruning of the abnormal hypervascularity with preserved flow to normal tissue — the desired endpoint.
Self-limited in days–weeks; warm compresses; photograph and follow
Skin necrosis / ulceration
<1%
Wound care; rarely surgical management
Transient post-procedure pain flare
10–30%
NSAIDs; usually resolves in 1–2 weeks
Groin hematoma / access-site complication
1–3%
Compression; thrombin injection if pseudoaneurysm
Hemarthrosis
Rare
Aspiration if large; self-limited usually
Infection / septic arthritis
Very rare
Antibiotics; joint aspiration
Deep vein thrombosis
<1%
Anticoagulation per routine
Contrast-induced nephropathy
Low (outpatient procedure, limited contrast)
Hydration; minimize contrast
Post-Procedure Care
Outpatient — discharge same day after 2–4 hours of observation.
Activity as tolerated; avoid strenuous activity for 1 week.
NSAIDs (if tolerated) for 1 week for expected post-embolization inflammation.
Photograph skin at discharge and at 2-week follow-up; patients instructed to call for any spreading redness, blistering, or ulceration.
Outcomes assessment: VAS and WOMAC at baseline, 1 month, 3 months, 6 months, 12 months.
Expected timeline: initial pain relief within 1–4 weeks; maximum benefit by 3 months; durability through 12–24+ months in responders.
Role of GAE in the Knee OA Algorithm
Not a replacement for conservative management (PT, weight loss, NSAIDs, intra-articular injections). GAE is indicated after these have failed.
Bridge to TKA or long-term alternative for non-surgical candidates — younger patients delaying surgery, medically frail patients avoiding surgery.
Compared to genicular nerve ablation (RFA / cryoablation): both target the pain pathway; GAE addresses the inflammatory driver, nerve ablation addresses the signal. Durability and comparative effectiveness are still being studied.
Not yet ACR-endorsed for first-line care; insurance coverage is variable. Expanding evidence base may shift guideline positioning.
Can be repeated if pain returns after an initial response.
Evidence Summary
Okuno Y et al (2015, 2017) — foundational series: established the imipenem/cilastatin technique and demonstrated sustained pain relief; over 70 patients with durable improvement at 2 years.
Bagla S et al GENESIS (JVIR 2020): first major US prospective trial with Embozene; VAS reduction ~60% sustained at 24 months; major complication rate 0%.
Landers SJ et al (Radiology 2023): first double-blind sham-controlled RCT — GAE outperformed sham for pain and WOMAC at 12 months in moderate-to-severe OA. Provides the highest-quality evidence to date.
Little MW et al (CVIR 2021) — systematic review: pooled 10 studies, 364 patients; consistent, clinically meaningful improvement; most AEs minor and self-limited.
SIR Clinical Pathways (2024 update): GAE is considered a promising option for appropriately selected knee OA patients who have failed conservative management; ongoing multicenter trials will clarify durability and comparative effectiveness.
References
Okuno Y, Korchi AM, Shinjo T, Kato S. Transcatheter arterial embolization as a treatment for medial knee pain in patients with mild to moderate osteoarthritis. Cardiovasc Intervent Radiol. 2015;38(2):336–343.
Okuno Y, Korchi AM, Shinjo T, Kato S, Kaneko T. Midterm clinical outcomes and MR imaging changes after transcatheter arterial embolization as a treatment for mild to moderate radiographic knee osteoarthritis resistant to conservative treatment. J Vasc Interv Radiol. 2017;28(7):995–1002.
Bagla S, Piechowiak R, Hartman T, Orlando J, Del Gaizo D, Isaacson A. Genicular artery embolization for the treatment of knee pain secondary to osteoarthritis. J Vasc Interv Radiol. 2020;31(7):1096–1102.
Bagla S, Piechowiak R, Sajan A, Orlando J, Hartman T, Isaacson A. Multicenter randomized sham controlled study of genicular artery embolization for knee pain secondary to osteoarthritis. J Vasc Interv Radiol. 2022;33(1):2–10.e2.
Landers S, Hely R, Page R, et al. Genicular artery embolization to improve pain and function in early-stage knee osteoarthritis: 12-month results of a randomized controlled trial. Radiology. 2023;308(3):e222303.
Little MW, Gibson M, Briggs J, et al. Genicular artery embolization in patients with osteoarthritis of the knee (GENESIS) using permanent microspheres: interim analysis. Cardiovasc Intervent Radiol. 2021;44(6):931–940.
Casadaban LC, Mauro DM, Solomon SB, et al. Safety and efficacy of genicular artery embolization: multicenter real-world experience. J Vasc Interv Radiol. 2024;35(5):652–660.
Padia SA, Genshaft S, Blumstein G, et al. Genicular artery embolization for the treatment of symptomatic knee osteoarthritis. JB JS Open Access. 2021;6(4):e21.00085.
Sajan A, Isaacson A, Bagla S. The role of genicular artery embolization in the management of knee pain. Semin Intervent Radiol. 2021;38(5):541–545.
Taslakian B, Swilling D, Attur M, et al. Genicular artery embolization for knee pain: mechanism, indications, and outcomes. Radiographics. 2023;43(8):e230001.
Full technique in RadCall Pro
Complete microcatheter matrix, particle sizing by vessel caliber, cone-beam CT protocol, and salvage strategies for non-target embolization available in RadCall Pro.