Elbow Stability
Primary stabilizers: Ulnohumeral articulation · anterior bundle of MCL (valgus stability) · LUCL (prevents PLRI).
Secondary stabilizers: Radiocapitellar articulation · common flexor-pronator tendon · common extensor tendon · joint capsule.
Key concept: Injury to primary stabilizers leads to elbow instability. Any fracture involving a primary stabilizer attachment site should prompt a search for associated ligament and soft-tissue injuries.
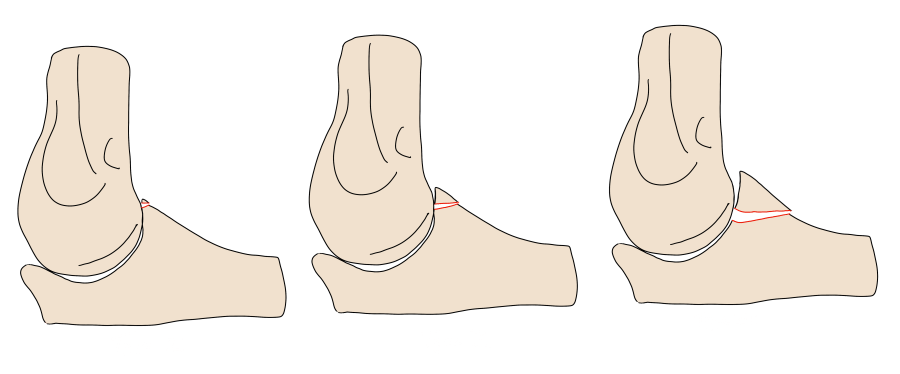
Distal Humerus — AO-ASIF Classification
Two-column concept: The medial column terminates at the medial epicondyle; the lateral column terminates at the lateral epicondyle and capitellum. Disruption of either column compromises structural stability. CT is recommended after radiographic identification given the high rate of surgically relevant injuries.
| AO-ASIF Type | Description | Management |
|---|---|---|
| A — Extraarticular | A1: epicondylar avulsion · A2: simple metaphyseal · A3: metaphyseal with comminution | Minimally displaced A1: conservative. Displaced avulsion, A2, A3: surgery |
| B — Partial articular (single column) | B1: lateral condylar (sagittal) · B2: medial condylar (sagittal) · B3: frontal articular (coronal shear — capitellum/trochlea) | Most require surgery. B1/B2 without comminution may trial conservative initially but usually require fixation |
| C — Complete articular (both columns) | C1: simple articular + simple metaphyseal · C2: simple articular + metaphyseal comminution · C3: articular + metaphyseal comminution | Surgery in medically fit patients |
Reporting Checklist — Distal Humerus
- Column involvement (medial, lateral, or both)
- Direction and displacement of any epicondylar avulsion
- Articular involvement and intraarticular extension
- Comminution or two-column injury
Coronoid Process — O'Driscoll Classification
The coronoid provides the anterior margin of the ulnohumeral joint, resists varus stress, and prevents posterior subluxation. Anteromedial facet involvement is particularly important — it confers valgus stability and is the MCL attachment site. CT with 3D reformats is recommended for all coronoid fractures.
| Type | Location | Significance |
|---|---|---|
| I — Tip | Coronoid tip (~1/3 of process) | Conservative if stable; instability risk increases with larger fragments. Even tiny tip fractures herald occult associated injuries (LUCL, lateral capsule) in the terrible triad setting |
| II — Anteromedial facet | Anteromedial facet ± sublime tubercle (MCL insertion) | Nearly always requires surgery — varus and posteromedial rotatory instability. Subtypes defined by degree of medial involvement and sublime tubercle involvement |
| III — Base | Base of coronoid (>50% of process) | Always surgical — major instability. Often seen with complex dislocations |
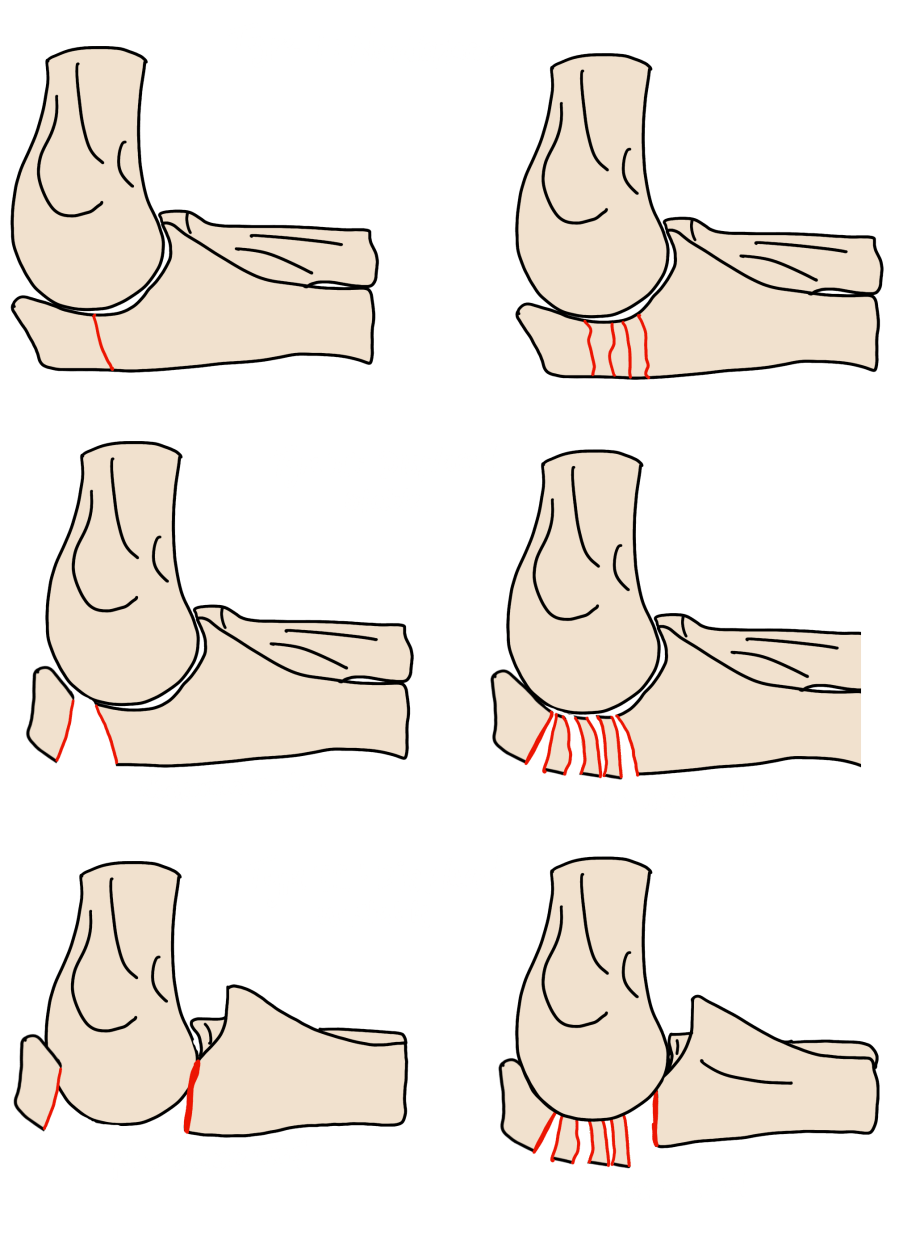
Olecranon — Mayo Classification
The olecranon forms the posteroinferior margin of the ulnohumeral joint, acts as a buttress against anterior dislocation, and is the triceps insertion site. Mechanism: axial load at 90° flexion or forceful hyperextension. Displacement greater than 2 mm warrants surgical consideration.
| Type | Description |
|---|---|
| Type 1 | Non-displaced (<2 mm gap, stable during flexion) |
| Type 2 | Displaced >2 mm, stable elbow |
| Type 3 | Displaced + elbow instability |
Reporting Checklist — Olecranon
- Degree of displacement (>2 mm or increases with flexion/extension = surgery)
- Comminution (favors plate fixation over tension band wiring)
- Coronoid process involvement (requires medial plate fixation to prevent instability)
- Fracture pattern: transverse (tension band), oblique (screw), comminuted (plate)
Radial Head — Mason-Johnston Classification
Radial head fractures are the most common elbow fracture in adults, accounting for 33–50% of all elbow fractures. Mechanism: fall on an outstretched hand (FOOSH) with forearm pronation and elbow in extension/flexion 0–80°. Subtle fractures are indicated by anterior and posterior fat pad elevation.
| Type | Description | Management |
|---|---|---|
| I | No or minimal (<2 mm) displacement | Conservative (sling, early ROM) |
| II | Displaced ≥2 mm, <30% articular surface | Conservative if ROM preserved; surgery if ROM is poor or articular surface involvement >30% |
| III | Comminuted, no dislocation | Surgery (ORIF or radial head replacement) |
| IV | Any radial head fracture + elbow dislocation | Surgery |
Reporting Checklist — Radial Head
- Degree of displacement (mm)
- Articular surface involvement (%)
- Comminution
- Associated dislocation (Mason-Johnston type IV)
- Search for associated injuries: coronoid fracture, MCL/LUCL tear, Essex-Lopresti (check DRUJ on wrist radiograph)
Essex-Lopresti Injury
Comminuted radial head fracture + DRUJ dislocation + interosseous membrane disruption, creating a "floating radius." Surgery is nearly always required.
Suspect when wrist pain accompanies a radial head fracture. Check the DRUJ on wrist radiographs — a radioulnar distance >5 mm compared to the contralateral side is diagnostic.
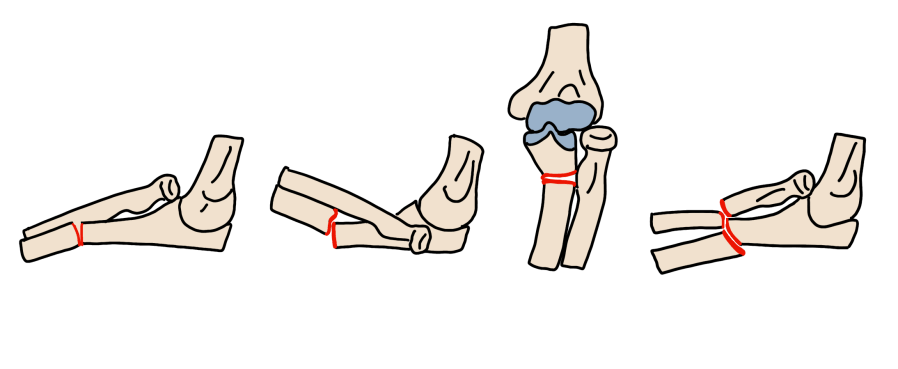
Elbow Dislocation
Elbow dislocation is the second most common joint dislocation in adults after the shoulder. Most dislocations are posterior. Classified as simple (no fracture) or complex (associated fracture). Mechanism: FOOSH with axial compression, supination, and valgus stress.
| Stage | Injury Pattern | Instability |
|---|---|---|
| I | LUCL + RCL damage | Posterolateral rotatory instability (PLRI) |
| II | Stage I + capsule + lateral soft tissues | Trochlea perched on coronoid (near-complete dislocation) |
| III | Stage II + anterior MCL bundle | Frank posterior dislocation with varus and valgus instability |
Drop sign: Ulnohumeral distance ≥4 mm on post-reduction lateral radiograph — may predict PLRI development.
Associated Injuries to Search For
- Radial head fracture (axial compression on capitellum)
- Coronoid fracture (shearing)
- Medial epicondyle fracture
- Flexor-pronator and brachialis muscle injuries
- MCL/LUCL tears
Terrible Triad
Posterior elbow dislocation + radial head fracture + coronoid fracture — extensive ligament damage leads to chronic instability if inadequately treated. Early surgical repair is critical.
Obtain CT if 2 of 3 components are identified on radiographs. Even a tiny coronoid tip fracture is significant in this setting. Evaluate the anteromedial facet on CT with 3D reformats.
Monteggia Fracture-Dislocation — Bado Classification
Ulnar fracture combined with radiocapitellar dislocation. All types require early surgical repair — delayed recognition leads to chronic instability. Suspect when any ulnar fracture is identified, as radiocapitellar dislocation can be missed if spontaneously reduced before imaging. CT is recommended to detect additional fractures.
| Type | Ulnar Fracture | Radial Head Dislocation | Notes |
|---|---|---|---|
| I (most common in adults) | Proximal/mid third, anterior apex angulation | Anterior | FOOSH or direct blow |
| II | Proximal/mid third, posterior apex angulation | Posterior | Direct blow to flexed forearm |
| III | Proximal ulnar metaphysis | Lateral | More common in children |
| IV | Proximal/mid third + radial shaft fracture | Anterior | Both-bone fracture variant |
Reference
Sheehan SE et al. Traumatic Elbow Injuries: What the Orthopedic Surgeon Wants to Know. RadioGraphics. 2013;33(3):869–888.