Finger Injuries
| Injury | Mechanism | Key Imaging Findings | Management |
|---|---|---|---|
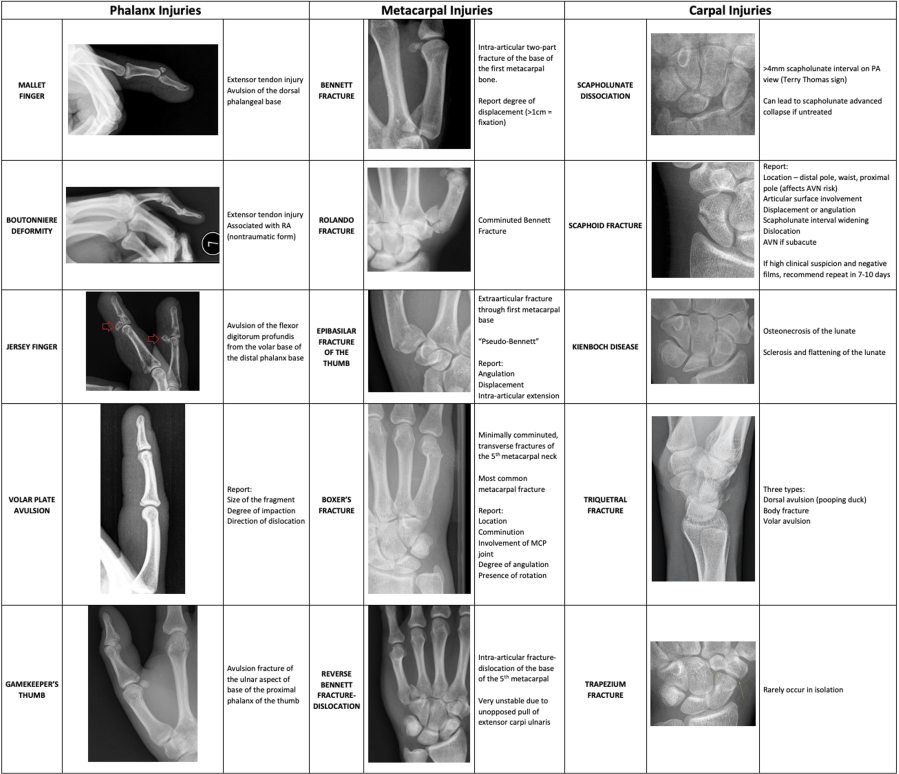
| Mallet finger | Forced DIP flexion during active extension (ball striking fingertip) | DIP flexion deformity; avulsion fracture at dorsal distal phalanx base (may be subtle). MRI: extensor tendon disruption at insertion | Splint DIP in extension 6–8 weeks. Surgery if: ≥50% articular surface involvement or volar subluxation of distal phalanx. Untreated → swan-neck deformity |
| Jersey finger | Forced extension during active DIP flexion (grabbing jersey). 75% ring finger | Osseous avulsion fragment at volar distal phalanx base (not always present). MRI: FDP tendon retraction — report level of retraction | All require surgery. Leddy-Packer: Type I retracted to palm (urgent <1 wk); Type II to PIP; Type III large fragment at DIP (within 3 wk) |
| Seymour fracture | Forced DIP flexion in children (door-slam) | Open physeal fracture of distal phalanx with dorsal angulation. Nail plate lies superficial to proximal nail fold; germinal matrix interposed between fragments | Surgical irrigation, nail plate removal, fracture reduction. If untreated: growth arrest, infection, deformity |
| Coach finger (PIP dorsal dislocation) | Forced hyperextension with axial load at PIP | Dorsal dislocation of PIP joint. Post-reduction: V sign (dorsal base of P2 separated from P1 head) = persistent subluxation/instability. Volar plate injury | Surgery if: irreducible, ≥40% articular surface fracture, persistent instability (V sign), or volar plate entrapment |
| Boutonnière deformity | Forced flexion or direct blow to PIP (central slip avulsion) | PIP flexion + DIP hyperextension. XR: may show avulsion at dorsal P2 base. MRI: central slip disruption with lateral band volar subluxation | Acute: splint PIP in extension. Surgery if osseous avulsion or laceration present. Chronic deformity: surgery |
| Volar plate avulsion | Hyperextension or dislocation, most common at PIP | Avulsion at distal attachment of volar plate; best seen on lateral XR. Type I: distal avulsion; Type II: surrounding soft tissue involvement; Type III: fracture-dislocation | Splint if stable. Surgery if: large fracture (≥40% articular surface), joint subluxation, or volar plate entrapment |
| Collateral ligament injury | Radial or ulnar deviation of extended finger | Ulnar/radial deviation or soft-tissue swelling on XR. MRI (coronal): disruption of low-signal ligament band with fluid signal. Exception: index finger RCL injuries are treated surgically | Most treated conservatively with buddy taping. Surgery for index finger RCL tears and complete tears failing conservative treatment |
| Pulley injury (climber's finger) | Powerful flexion (rock climbing). A2 most common | MRI (sagittal): increased signal/disruption within pulley fibers. Bowstringing: increased flexor tendon–bone distance (A2 = proximal phalanx level; A4 = middle phalanx). US demonstrates bowstringing dynamically | Surgery for A2 if bowstringing extends proximal to P1 base (= complete disruption). Otherwise conservative |
Metacarpal Fractures
| Location | Key Points | Surgical Thresholds |
|---|---|---|
| Metacarpal neck (Boxer fracture = 5th MC) | Most common MC fracture (5th MC). Apex dorsal angulation. Check for rotational malalignment (finger scissoring on clinical exam) | Max tolerated angulation by finger: index 10°, long 15°, ring 30°, small 40°. Rotational deformity = surgery |
| Metacarpal shaft | Transverse (direct blow), oblique/spiral (torque). Spiral fractures are often unstable | Max angulation: index/long 0°, ring 20°, small 30°. Surgery if: irreducible, open, multiple fractures, rotational deformity |
| Metacarpal base | Forced flexion at wrist with arm extended; commonly associated with CMC dislocations. Evaluate with lateral/oblique views and CT if needed | Intraarticular: surgery if malaligned (>20% articular surface). Displaced CMC fracture-dislocations = surgery |
Thumb Injuries
| Injury | Key Imaging Findings | Management |
|---|---|---|
| Bennett fracture | Two-part oblique intraarticular fracture of thumb MC base with metacarpal subluxation. Axial loading on partially flexed thumb | Percutaneous pinning if anatomic reduction achievable; otherwise ORIF |
| Rolando fracture | Comminuted intraarticular fracture of thumb MC base (T or Y pattern). Same mechanism as Bennett but higher energy | ORIF required for all |
| Gamekeeper thumb (UCL injury) | Forced radial deviation of thumb MCP. XR: subtle subluxation, small avulsion. MRI/US: UCL tear; Stener lesion = UCL retracted superficial to adductor aponeurosis ("yo-yo on a string" on MRI) — will NOT heal without surgery. DO NOT perform stress views — may create Stener lesion | Partial tears: immobilization. Complete UCL tears and Stener lesions: surgical repair |
Distal Phalanx Tuft Fractures
Most common hand fracture. Usually stable. Report if displaced — implies nailbed injury (open fracture requiring nail plate removal and nailbed repair). Base fractures are unstable and require surgery. Widening of fracture line on lateral view = nail bed entrapment between fragments.
Pathologic Hand Fractures
Most common underlying lesion is enchondroma — lucent lesion with lobular sclerotic margin, endosteal scalloping, ring-and-arc mineralization in tubular bones of hand. Other causes: aneurysmal bone cyst, giant cell tumor, epidermoid inclusion cyst. Chondrosarcoma rare but suspect if extensive endosteal scalloping, cortical breakthrough, or soft-tissue component.
Distal Radius Fracture Reporting Checklist
- Loss of volar tilt
- Loss of radial inclination
- Shortening relative to ulna
- Intraarticular extension
- Articular diastasis/depression
- Comminution
- Ulnar styloid fracture — location, displacement; if base fracture check DRUJ/TFCC integrity
- Disruption of carpal arcs

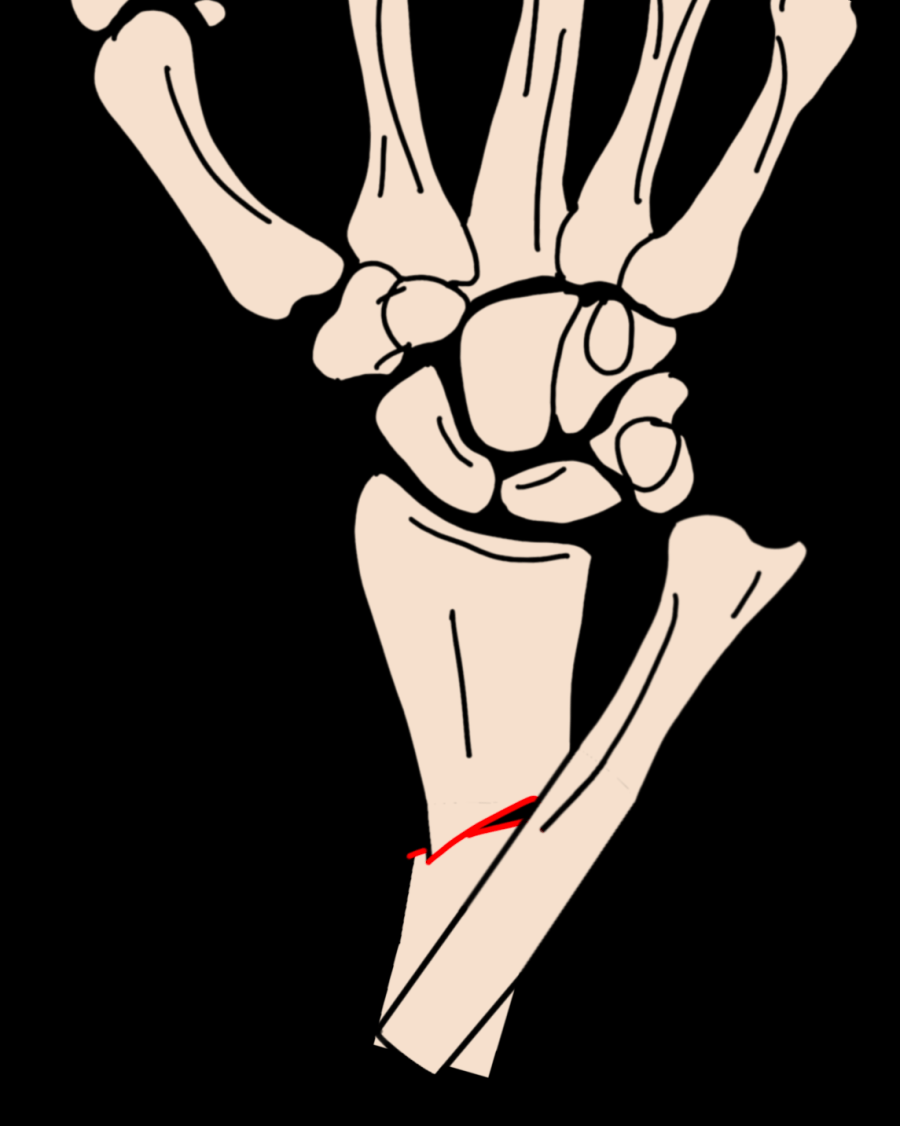
Galeazzi Fracture-Dislocation
Radial fracture combined with DRUJ dislocation. Type I: dorsal displacement; Type II: volar displacement. Always assess the DRUJ when a distal radius fracture is identified.
Essex-Lopresti Injury
Radial head fracture combined with DRUJ dislocation and interosseous membrane rupture. Assess the DRUJ on wrist XR whenever a radial head fracture is present.
Reference
Wieschhoff GG, Sheehan SE, et al. Traumatic Finger Injuries: What the Orthopedic Surgeon Wants to Know. RadioGraphics. 2016;36(4):1106–1128.