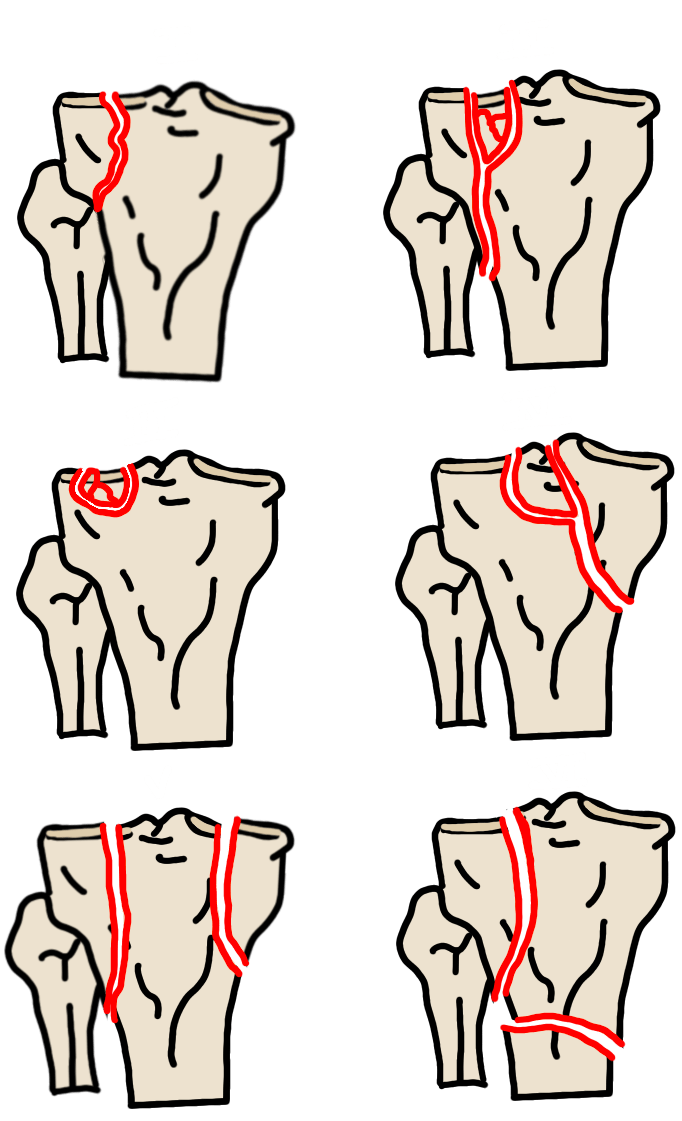
Schatzker Classification
| Type | Description | Management Notes |
|---|---|---|
| I | Lateral split — pure split fracture, no depression | Younger patients with good bone quality; ORIF if displaced |
| II | Lateral split + depression | Most common surgical type; ORIF with bone grafting |
| III | Focal depression only — no split | Elderly or osteoporotic patients; ORIF and bone graft for >5 mm depression |
| IV | Medial plateau — split or depression | High-energy injury; risk of popliteal vascular injury; ligamentous injury common |
| V | Bicondylar — both plateaus involved | High-energy; dual incision ORIF |
| VI | Bicondylar + metaphyseal dissociation | Most severe; tibia shaft dissociated from metaphysis; staged with external fixator then ORIF |
Surgical Thresholds
Surgical intervention is generally considered when:
- Articular diastasis ≥3–4 mm, or
- Articular depression ≥4–5 mm
These are relative thresholds and should be interpreted in the context of patient age, activity level, and bone quality. Always measure and report articular step-off in millimeters.
Contralateral joint space widening relative to the normal compartment indicates ligamentous injury on the uninjured side.
Reporting Checklist
- Fracture morphology: split, depressed, or bicondylar
- Articular step-off: measure in mm (surgical threshold typically ≥3–5 mm)
- Contralateral joint space widening (indicates ligamentous injury)
- Intraarticular loose bodies
- Associated injuries (see below)
Associated Injuries
Tibial spine avulsion: Associated with ACL, MCL, and medial meniscus injuries. If identified on radiograph, recommend MRI for ligamentous assessment.
Deep notch sign: Impaction of the lateral femoral condyle cortex seen on lateral radiograph or sagittal CT — associated with ACL injury.
Fibular head fracture: Raises concern for peroneal nerve injury (foot drop) and posterolateral corner injury.
Fibular shaft fracture: Image the ipsilateral ankle to exclude a Maisonneuve fracture pattern.
Popliteal artery injury: Most relevant with Schatzker IV fractures and knee dislocation. Obtain CTA if vascular compromise is suspected clinically.