Varicocele Embolization — Sclerotherapy and Coil Technique
Percutaneous transvenous embolization of the internal spermatic (gonadal) vein is the image-guided alternative to surgical varicocelectomy. Using retrograde venography from a jugular or femoral approach, the gonadal vein and accessory collaterals are occluded with coils, sclerosant foam, or glue — eliminating reflux while avoiding general anesthesia and scrotal dissection.
Key points
Indications: palpable varicocele with infertility (abnormal semen parameters), symptomatic scrotal pain, adolescent testicular growth arrest, and post-surgical recurrence. Subclinical (imaging-only) varicocele alone is generally not an indication.
Left-sided predominance (~90%): the left gonadal vein drains at a right angle into the left renal vein and lacks competent valves in ~40%; isolated right varicocele raises concern for retroperitoneal mass and warrants cross-sectional imaging.
Dubin–Amelar grading (clinical): Grade I palpable only with Valsalva, Grade II palpable at rest, Grade III visible through scrotal skin — all grades are candidates for embolization if symptomatic.
Access: right internal jugular or right common femoral vein; IJ access provides a more favorable angle into the left renal vein and gonadal vein origin.
Embolic agents: pushable or detachable coils (most common in US), sodium tetradecyl sulfate (STS) foam sclerosant, Amplatzer plugs, and n-BCA glue — often combined ("sandwich" technique: distal sclerosant + proximal coils) to occlude the main trunk and collaterals.
Outcomes: technical success 90–95%; semen parameter improvement 60–70%; pregnancy rates comparable to surgical ligation; recurrence 4–11% (higher with coils alone than sclerosant–coil combination).
Dull ache worse with standing/exertion, relieved supine; exclude other causes (epididymitis, hernia)
Adolescent testicular growth arrest
Ipsilateral testicular volume >20% smaller than contralateral on serial ultrasound
Recurrence after surgical ligation
Embolization is preferred salvage — targets missed collaterals that caused recurrence
Patient preference
No general anesthesia, no scrotal incision, faster return to activity vs surgery
Type
Contraindication
Absolute
Uncorrectable coagulopathy · Severe contrast allergy not premedicable · Active bacteremia
Relative
Subclinical varicocele without infertility or symptoms · Severe renal impairment (contrast load) · Unfavorable gonadal vein anatomy (multiple small channels not amenable to catheterization — consider antegrade or surgical)
Relevant Anatomy
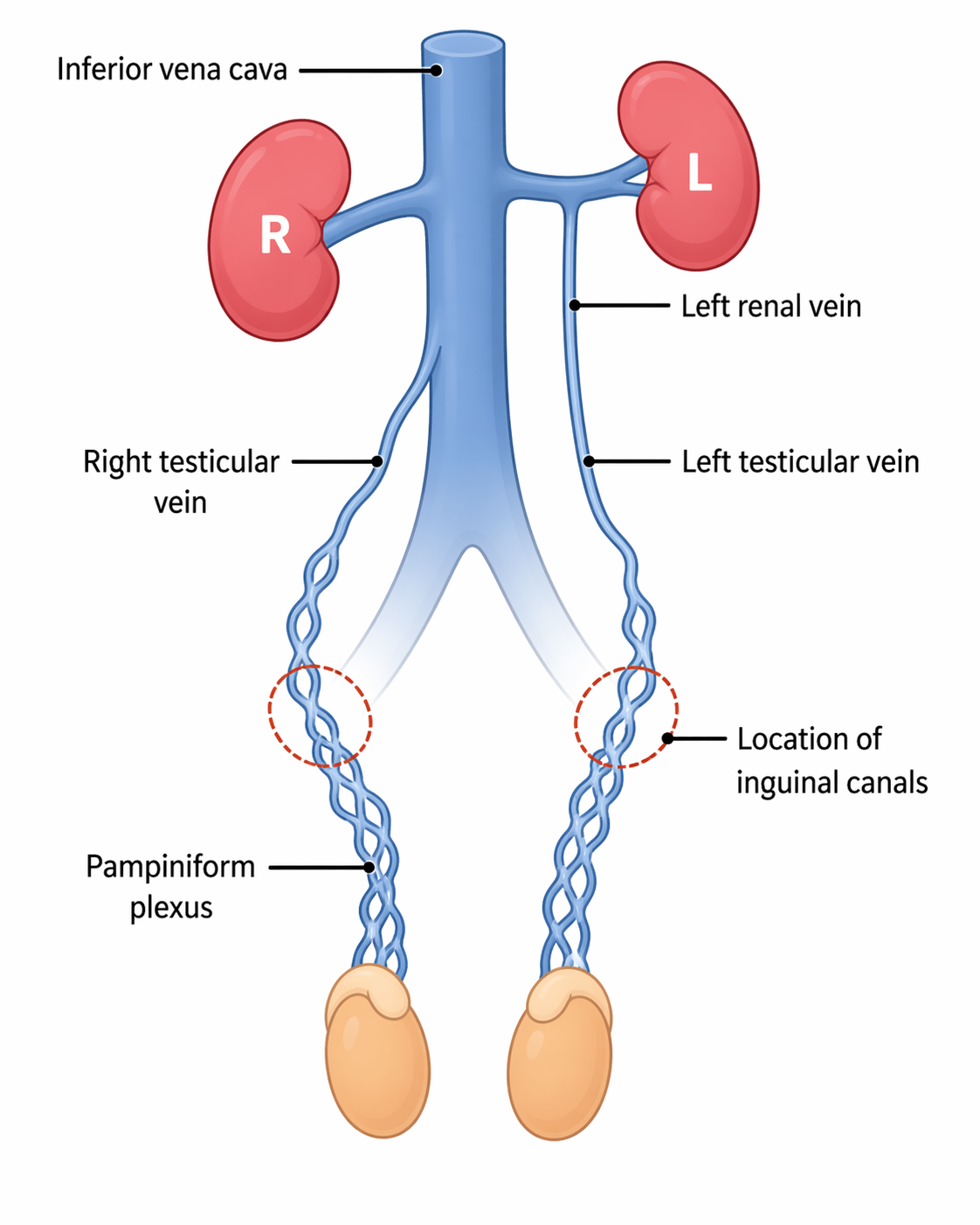
The internal spermatic (gonadal, testicular) vein is the target vessel. Anatomic asymmetry drives the disease:
Left gonadal vein: drains into the left renal vein at a near-perpendicular angle; longer column of blood; valvular incompetence in ~40%; nutcracker compression of the left renal vein can contribute.
Right gonadal vein: drains directly into the IVC (80–90%) at an oblique angle; rarely into the right renal vein (10–20%); lower hydrostatic load and fewer varicoceles.
Collateral networks: periureteric, retroperitoneal, capsular renal, and transcrotal cross-collaterals are the main cause of recurrence and must be identified on venography and occluded.
Testicular vein anatomy — left gonadal vein drains into the left renal vein at a right angle; right gonadal vein drains obliquely into the IVC. This asymmetry explains the ~90% left-sided predominance of varicoceles.
Clinical Grading — Dubin and Amelar
Grade
Clinical Finding
Grade I
Palpable only with Valsalva maneuver
Grade II
Palpable at rest without Valsalva
Grade III
Visible through scrotal skin ("bag of worms")
Subclinical
Detected only by ultrasound or venography — generally not embolized unless part of infertility workup with strong indication
Sonographic Criteria
Pampiniform plexus veins >3 mm in diameter
Reflux >1 second on Valsalva (color or spectral Doppler)
Examination in standing position (supine alone underestimates)
Color Doppler ultrasound demonstrating dilated pampiniform plexus veins >3 mm with venous reflux — characteristic of a left varicocele.Color Doppler ultrasound showing dilated pampiniform plexus veins — venous flow confirmed on color signal without spectral waveform acquisition.
Isolated right-sided varicocele: uncommon; obligates cross-sectional imaging of the abdomen to exclude retroperitoneal mass, renal cell carcinoma with IVC tumor thrombus, or situs anomaly compressing the right gonadal vein.
Procedure Overview
The following is a high-level summary. Full catheter and microcatheter selection, coil sizing, sclerosant foam preparation ratios, and collateral mapping algorithms are available in RadCall Pro.
Access and Catheterization
Access: right internal jugular vein (preferred for left gonadal vein — favorable angle) or right common femoral vein. 5–6 Fr sheath.
Left renal vein catheterization: 5 Fr cobra, multipurpose, or reverse-curve (SOS, Simmons) catheter; selective left renal venogram to localize the gonadal vein ostium (typically inferior aspect of the left renal vein, 1–2 cm from IVC).
Gonadal vein catheterization: advance microcatheter through guiding catheter into the gonadal vein; perform diagnostic venogram with Valsalva to confirm reflux and map collaterals (periureteric, capsular renal, cross-pelvic).
Right-side approach: direct IVC catheterization; right gonadal vein origin is smaller and more obliquely oriented — reverse-curve catheters are often required.
Embolization Strategy
Distal embolization first: advance microcatheter to near the inguinal canal (just above the internal ring); deploy coils, plug, or inject STS foam to occlude the distal gonadal vein and pampiniform plexus inflow.
Collateral occlusion: identify and embolize parallel channels (periureteric, retroperitoneal); skipping these is the leading cause of recurrence.
Proximal coil anchor: deploy coils in the proximal gonadal vein near (but not at) the renal vein ostium to prevent coil migration into the renal vein or IVC.
Completion venogram: confirm stasis, no residual reflux on Valsalva, and no non-target filling.
Gonadal vein venogram pre-embolization — dilated internal spermatic vein with contrast filling of the pampiniform plexus confirming reflux.
Embolic Agent Selection
Agent
Advantages
Limitations
Coils (pushable/detachable)
Precise placement; durable; widely available
Miss small collaterals; more expensive; recurrence if collaterals untreated
STS foam sclerosant (3% STS + air, 1:4 ratio)
Penetrates small collaterals; inexpensive; excellent for distal pampiniform plexus
Risk of non-target embolization if not contained; transient scrotal pain
Amplatzer vascular plug
Single device occlusion of main trunk; lower device cost vs coils
Requires 4–6 Fr catheter delivery; not for small or tortuous veins
n-BCA glue
Penetrates collaterals; fast
Operator-dependent; catheter adherence risk
Sandwich technique (STS + coils)
Lowest recurrence in comparative series
Longer procedure
Complications
Complication
Rate
Management
Recurrence / persistent reflux
4–11%
Most common outcome failure; re-embolization targeting missed collaterals
Scrotal pain / thrombophlebitis
5–15%
Usually transient 2–7 days; NSAIDs, scrotal support; related to sclerosant effect
Coil migration
<1%
Most migrate to pulmonary circulation and are asymptomatic; snare retrieval if large or symptomatic; prevented by proper sizing and anchor placement distal to renal vein
Avoided by distal microcatheter position and Valsalva during sclerosant injection
Hydrocele
<1% (much lower than surgical)
Conservative; aspiration if symptomatic
Post-Procedure Care
Same-day discharge after 2–4h of bed rest (jugular or femoral access).
Activity: light activity day 1–2; resume full activity at 3–5 days.
Symptom expectations: transient scrotal ache and low-grade fever 2–7 days (post-embolization syndrome); treat with NSAIDs and scrotal support.
Follow-up: scrotal ultrasound at 3 months for residual reflux; semen analysis at 3 and 6 months for infertility indication.
Pregnancy counseling: semen parameter improvement peaks at 3–6 months; pregnancy rates approach surgical outcomes by 12 months.
Evidence Summary
Halpern J et al (2016, J Vasc Interv Radiol): embolization vs microsurgical varicocelectomy — equivalent pregnancy rates (~30–40%) and semen improvement; embolization had faster recovery and no anesthesia.
Iaccarino V & Venetucci P (2012, CVIR): 30-year series; technical success 95%; recurrence <5% with combined sclerosant + coil technique.
Nabi G et al (2004, Acta Radiol) meta-analysis: percutaneous embolization and open ligation have comparable efficacy; embolization has lower complication rate.
Makris GC et al (2018, CVIR): foam sclerotherapy alone and sandwich technique achieve lower recurrence than coils alone.
References
Halpern J, Mittal S, Pepe K, et al. Percutaneous embolization of varicocele: technique, indications, relative contraindications, and complications. Asian J Androl. 2016;18(2):234–238.
Iaccarino V, Venetucci P. Interventional radiology of male varicocele: current status. Cardiovasc Intervent Radiol. 2012;35(6):1263–1280.
Makris GC, Efthymiou E, Little M, et al. Safety and effectiveness of the different types of embolic materials for the treatment of testicular varicoceles: a systematic review. Br J Radiol. 2018;91(1088):20170445.
Nabi G, Asterlings S, Greene DR, Marusic L. Percutaneous embolization of varicoceles: outcomes and correlation of semen improvement with pregnancy. Urology. 2004;63(2):359–363.
Kroencke TJ, et al. Radiologic treatment of varicoceles: technique and results. RadioGraphics. 2002;22:e1.
Flacke S, Schuster M, Kovács A, et al. Embolization of varicoceles: pretreatment sperm motility predicts later pregnancy in partners of infertile men. Radiology. 2008;248(2):540–549.
Jargiello T, Drelich-Zbroja A, Falkowski A, et al. Endovascular transcatheter embolization of recurrent postsurgical varicocele: anatomic reasons for surgical failure. Acta Radiol. 2015;56(1):63–69.
Full technique in RadCall Pro
Complete catheter and microcatheter selection, coil sizing tables, STS foam preparation ratios, collateral mapping algorithms, and sandwich-technique protocols are available in RadCall Pro.