Balloon-occluded retrograde transvenous obliteration (BRTO) is the definitive endovascular treatment for gastric varices — retrograde catheterization of the gastrorenal or gastrocaval shunt, balloon occlusion to allow sclerosant pooling, and direct obliteration of varices with preservation of portal perfusion.
Key points
BRTO is the treatment of choice for gastric varices (fundal type, GOV2 and IGV1) — superior to TIPS for isolated gastric varices with preserved liver function and requires a gastrorenal shunt (present in ~85% of gastric varix patients).
Gastrorenal shunt (GRS) is the anatomic prerequisite — the shunt provides retrograde catheter access to the varices. GRS absent in ~15%; alternative: gastrocaval shunt (BRTO from IVC), or TIPS as alternative therapy.
After BRTO, esophageal varices worsen in ~40% — portal pressure increases as shunted blood is redirected into the portal system. Screen for and treat esophageal varices before BRTO; plan endoscopic banding program post-procedure.
PARTO (plug-assisted retrograde transvenous obliteration) uses a vascular plug instead of a balloon, allowing faster sclerosant delivery and same-session completion; CARTO (coil-assisted) uses coils for similar purposes — both are modern BRTO variants without prolonged balloon dwell time.
Sclerosant options: Ethanolamine oleate (EO, preferred in Japan/Korea), sodium tetradecyl sulfate (STS) foam (preferred in US/Europe). Both achieve >90% gastric varix obliteration at 1 year.
Technical success >95%; gastric varix obliteration at 1 year >90% in published series. Rebleeding rate <5% after successful obliteration.
Indications
Indication
Class
Notes
Acute gastric variceal bleeding — active or recent hemorrhage
Urgent
BRTO preferred over TIPS for isolated gastric varices if GRS present; TIPS preferred if concurrent esophageal varices or hepatic encephalopathy
Secondary prevention of gastric variceal rebleeding
Elective
Standard of care for GOV2 and IGV1 with GRS
Primary prophylaxis (large gastric varices with red signs)
Conditional
Shared decision with hepatology; less established than for esophageal varices
Hepatic encephalopathy refractory to medical management due to portosystemic shunt
Elective
BRTO of large spontaneous portosystemic shunts; may dramatically improve HE
Gastric varices not amenable to endoscopic cyanoacrylate injection
Rescue
When endoscopy fails or is not available
Contraindications
Type
Contraindication
Absolute
Absent gastrorenal or gastrocaval shunt (no retrograde access) · Child-Pugh C with MELD >20 and no transplant plan · Severe portal vein thrombosis (main PVT) limiting ability to tolerate increased portal pressure
Relative
Active esophageal varices requiring treatment (band ligation first, or plan concurrent TIPS) · Severe ascites (BRTO increases portal pressure — ascites may worsen) · Prior significant reaction to sclerosant · Significant renal impairment with EO (EO is nephrotoxic at high doses)
Relevant Anatomy
Gastric varices form from portal hypertension with retrograde flow through the left gastric and short gastric veins into the fundal varix network. The varices drain via spontaneous portosystemic shunts — the anatomy of the draining shunt determines BRTO access and approach.
Femoral or transjugular → IVC → inferior phrenic vein
Gastrohepatic shunt
Rare
Fundal varices → hepatic vein
Transhepatic approach or TIPS combination
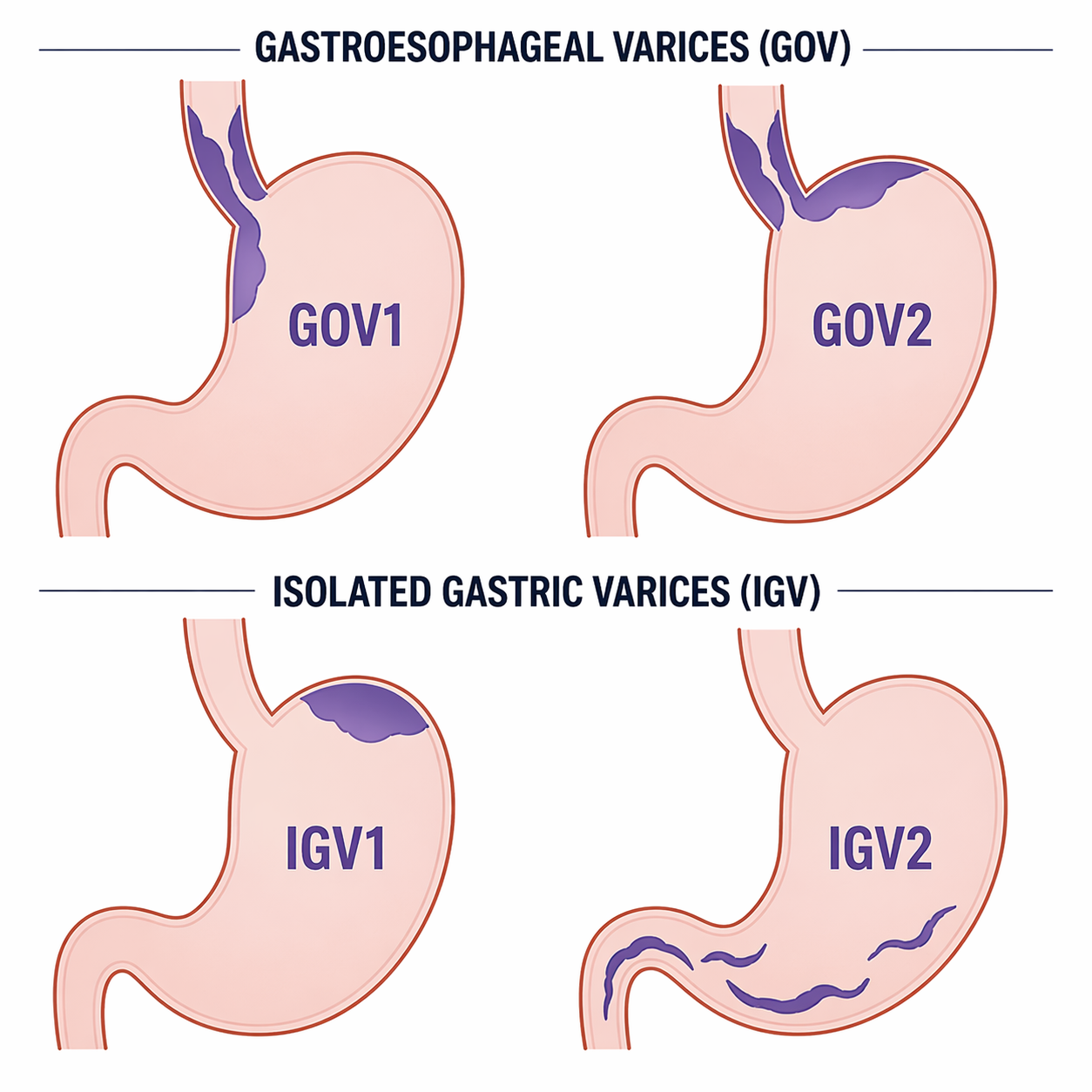
Sarin Classification of Gastric Varices
Sarin classification of gastric varices: GOV1 and GOV2 are continuous with esophageal varices; IGV1 and IGV2 are isolated. BRTO is the primary treatment for GOV2 and IGV1 when a gastrorenal shunt is present.
Type
Location
BRTO Target?
GOV1
Cardia, along lesser curvature — continuous with esophageal varices
No — treat as esophageal varices; band ligation preferred
GOV2
Fundal, along greater curvature — extends to fundus
Key principle: BRTO obliterates gastric varices by blocking their venous drainage (occlude GRS with balloon or plug) and injecting sclerosant retrograde into the varix bed. The blood stagnates and is sclerosed. Portal blood that previously bypassed the liver through the shunt is redirected into the portal circulation — this increases portal pressure but improves hepatic perfusion and function.
BRTO Variants
Technique
Occlusion Device
Duration
Key Advantage
Classic BRTO
Compliant occlusion balloon catheter in GRS
4–24h balloon dwell with sclerosant; patient admitted overnight
Gold standard; longest track record; sclerosant retained in varix bed
PARTO (plug-assisted RTO)
Amplatzer vascular plug occludes GRS
Same session; no prolonged dwell
Faster; no overnight balloon; plug permanent; same efficacy
CARTO (coil-assisted RTO)
Microcoils deployed in GRS before sclerosant
Same session
Similar to PARTO; coils + foam efficient combination
MBRTO (modified)
Balloon + microcoils to seal collaterals
Variable
For cases with multiple drainage pathways (GRS + gastrocaval)
Procedure Overview
The following is a high-level summary. Full balloon catheter sizing and positioning in the gastrorenal shunt, sclerosant preparation and injection volumes, collateral occlusion strategy, and PARTO/CARTO plug or coil selection are available in RadCall Pro.
Pre-Procedure Planning
Pre-procedure CT: CT of abdomen/pelvis with venous phase (portal venous phase); map GRS anatomy, shunt diameter, length, and identify all collateral drainage pathways. Shunt diameter determines balloon sizing.
Access: Right transjugular (IJV → IVC → left renal vein → GRS) OR right femoral (IVC → left renal vein → GRS).
Catheterization and Occlusion
Left renal vein catheterization: Catheter to left renal vein; CO2 or iodinated venogram to identify GRS origin from left renal vein
GRS catheterization: Advance balloon catheter (sizing 1 mm larger than GRS diameter) into GRS via guidewire; position beyond the junction of GRS and left renal vein
Balloon inflation: Inflate to occlude GRS; venogram through catheter lumen to confirm occlusion and varix filling; identify all collateral drainage veins (may need coil embolization of collaterals to keep sclerosant from escaping)
Collateral embolization: Coil any accessory drainage veins that would allow sclerosant escape before injection
Sclerosant Injection and Completion
Sclerosant injection: Inject EO or STS foam slowly under fluoroscopy until varices are filled; confirm opacification of fundal varix network. For classic BRTO: leave balloon inflated 4–12h with sclerosant retained; patient to ICU.
Balloon removal (classic BRTO): At 4–12h, deflate balloon and confirm stasis in varix bed; remove
For PARTO: Deploy Amplatzer plug in GRS, inject sclerosant, completion venogram; same session
Post-procedure CT: 48–72h CT to confirm varix obliteration and no early complications (pulmonary emboli from EO)
Complications
Complication
Rate
Management
Pulmonary EO embolism (if ethanolamine oleate used)
5–15% (usually asymptomatic)
Pre-treat with haptoglobin (Japan) and steroids; limit EO to <0.4 mL/kg; most clinically insignificant
Esophageal varix worsening
30–40%
Endoscopic band ligation post-BRTO; surveillance endoscopy 1–3 months
Ascites worsening
10–20%
Portal pressure increase; diuretics; rarely need TIPS
Pleural effusion (left-sided)
10–15%
Related to sclerosant effect near diaphragm; usually self-limiting
Fever / abdominal pain
Common
Post-embolization syndrome; NSAIDs, supportive care
Balloon rupture
Rare
Use properly sized balloons; have backup catheters
GRS thrombosis extending into renal vein
Rare
Anticoagulation; monitoring; usually resolves
Rebleeding
<5% after successful obliteration
Re-BRTO or TIPS
Esophageal varix surveillance is mandatory post-BRTO: Because BRTO redirects portosystemic shunt flow back into the portal system, portal pressure rises and esophageal varices develop or worsen in up to 40% of patients. EGD at 1 month is standard; early band ligation prevents hemorrhage.
Post-Procedure Care
Admission: Admit post-procedure for overnight monitoring (longer for classic BRTO with balloon dwell)
EGD at 1 month: Baseline assessment of esophageal varices post-BRTO; banding if high-grade
CT or MRI at 3 months: Confirm varix obliteration; portal vein patency; exclude complications
Hepatic function monitoring: BRTO may improve hepatic function (redirecting blood to portal circulation); watch for ascites worsening
Long-term: EGD every 6–12 months; hepatology co-management for underlying cirrhosis and liver disease progression
Anticoagulation: No anticoagulation routinely post-BRTO
MELD trend: BRTO often associated with MELD improvement (1–3 points) at 3–6 months due to improved hepatic perfusion
Evidence Summary
Cho SK et al (2015, Radiology): 97 patients; technical success 96%; varix obliteration 93% at 6 months; rebleeding 3%; esophageal varix worsening 34%.
Saad WE (2013, Semin Intervent Radiol): Comprehensive BRTO review; technical success >95%; rebleeding <5%; preferred over TIPS for isolated gastric varices with GRS.
Gwon DI et al (2015): PARTO vs BRTO outcomes comparable; PARTO faster; no need for prolonged balloon dwell.
Kim YH et al: BRTO vs TIPS for gastric varices — BRTO had significantly lower rebleeding for isolated fundal varices; TIPS preferred for concurrent esophageal varices or HE.
Luo X et al (2022 meta-analysis): BRTO vs TIPS for gastric varices: BRTO superior for gastric varix obliteration; TIPS superior for HE reduction. Patient selection critical.
Key principle: BRTO improves hepatic encephalopathy by eliminating the large portosystemic shunt (porto-systemic encephalopathy) — a major benefit in patients with refractory HE and spontaneous shunts.
References
Cho SK, et al. Balloon-occluded retrograde transvenous obliteration of gastric varices: outcomes and complications in 97 patients. AJR. 2015;204(6):1324–1334.
Saad WE. Balloon-occluded retrograde transvenous obliteration of gastric varices: concept, basic techniques, and outcomes. Semin Intervent Radiol. 2012;29(2):118–128.
Gwon DI, et al. Vascular plug-assisted retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy: a prospective multicenter study. J Vasc Interv Radiol. 2015;26(11):1589–1595.
Luo X, et al. BRTO versus TIPS for gastric varices: a systematic review and meta-analysis. J Vasc Interv Radiol. 2022;33(7):815–825.
Kim YH, et al. Comparison of outcomes of balloon-occluded retrograde transvenous obliteration and transjugular intrahepatic portosystemic shunt for treatment of gastric varices. J Vasc Interv Radiol. 2014;25(6):959–963.
Takuma Y, et al. Balloon-occluded retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy: long-term follow-up. J Gastroenterol Hepatol. 2010;25(12):1904–1911.
Garcia-Pagan JC, et al. Use of early-TIPS for high-risk variceal bleeding. N Engl J Med. 2010;362(25):2370–2379.
Full technique in RadCall Pro
Complete balloon catheter sizing and GRS positioning, sclerosant preparation and injection volumes, collateral occlusion strategy, and PARTO/CARTO plug and coil selection available in RadCall Pro.