Bronchial artery embolization (BAE) is the first-line treatment for massive and recurrent non-massive hemoptysis. Hemoptysis originates from the systemic bronchial circulation in ~90% of cases — not the pulmonary arteries — because chronic inflammation, infection, or malignancy induces hypertrophy and neovascularization of bronchial and non-bronchial systemic arteries. Transcatheter embolization occludes these abnormal vessels at capillary level with particles, achieving immediate bleeding control in 70–99% of patients while preserving lung function.
Key points
Massive hemoptysis definition: >300–600 mL in 24 hours, or any rate causing airway compromise or hemodynamic instability. Mortality without treatment approaches 50–100%; BAE reduces in-hospital mortality to <10%.
CT angiography is essential pre-procedure — identifies bleeding side, vessel caliber (>2 mm abnormal), origin variants, and non-bronchial systemic supply. Skipping CTA risks missing the culprit vessel and causing non-target embolization.
Anterior spinal artery is the critical safety concern — arises from a common intercostobronchial trunk in ~5–10% and may co-originate with bronchial arteries. Inadvertent embolization causes devastating anterior cord infarction (paraplegia).
PVA particles 300–700 μm are standard embolic — large enough to avoid capillary-level bronchopulmonary shunts but small enough to occlude neovessels.
Immediate control 70–99%; recurrence 10–55% (highest in cystic fibrosis, aspergilloma, chronic TB). Recurrence is managed by repeat embolization or surgical resection of the culprit lung.
Etiology of Hemoptysis
Cause
Mechanism
Bronchiectasis (non-CF)
Most common cause worldwide; chronic airway inflammation → bronchial artery hypertrophy and neovascularization
Cystic fibrosis
Up to 9% of CF patients experience massive hemoptysis; high recurrence after BAE
Tuberculosis (active or post-treatment)
Most common cause in endemic regions; cavitary disease, post-TB bronchiectasis, aspergilloma
Aspergilloma / chronic pulmonary aspergillosis
Fungus ball in cavitary lung; friable neovessels at interface
Lung malignancy
Central tumors with bronchial invasion; bleeding may be arterial or venous; higher rebleeding after BAE
Cryptogenic (~10–15%)
No cause identified after full workup
Bronchial Artery Anatomy
Bronchial arteries typically arise from the descending thoracic aorta between T5 and T6 vertebral bodies. Branching patterns are highly variable — Cauldwell classified four major patterns:
Cauldwell Type
Pattern
Frequency
Type I
Intercostobronchial trunk (right) + two left bronchial arteries
~40%
Type II
Intercostobronchial trunk (right) + one left bronchial artery
~21%
Type III
Intercostobronchial trunk + right bronchial artery + two left bronchial arteries
~21%
Type IV
Intercostobronchial trunk + right bronchial artery + one left bronchial artery
~10%
Ectopic origins (~8–35% depending on series) include aortic arch, subclavian, internal mammary, brachiocephalic, thyrocervical trunk, costocervical trunk, and coronary arteries. Always perform a full descending thoracic aortogram to identify ectopic vessels that are missed on selective catheterization alone.
Bronchial artery anatomy — typical origins from the descending thoracic aorta at T5–T6, Cauldwell branching patterns, and the intercostobronchial trunk. Key: RBA = right bronchial artery · LBA = left bronchial artery · ICBT = intercostobronchial trunk · ICA = intercostal artery.
The Anterior Spinal Artery — Critical Safety
Adamkiewicz watchpoint: The artery of Adamkiewicz (dominant anterior radiculomedullary artery) arises from a left T9–T12 intercostal in ~75% of patients but can originate anywhere from T5 to L2. The anterior spinal artery commonly shares an origin with the right intercostobronchial trunk — the most frequent bronchial artery origin. A classic "hairpin" or "saw-tooth" midline vessel on selective injection indicates radiculomedullary branch supply and mandates microcatheter superselection distal to the spinal branch before embolization. When in doubt, do not embolize — re-position and re-image. Particle reflux into this pathway causes anterior cord infarction and permanent paraplegia.
Selective intercostal angiogram showing the classic midline "hairpin" configuration of the anterior spinal artery arising from a radiculomedullary branch — mandates microcatheter superselection distal to this branch before embolization.
Indications and Contraindications
Indication
Notes
Massive hemoptysis
>300–600 mL/24 h or airway compromise/hemodynamic instability — emergent BAE
Submassive hemoptysis with bleeding source identified
100–300 mL/24 h; elective BAE to prevent progression
Recurrent minor hemoptysis
Repeated episodes impairing quality of life or with CT evidence of hypertrophied bronchial arteries
Pre-surgical stabilization
BAE to achieve bleeding control prior to definitive lobectomy/pneumonectomy
Inability to avoid spinal artery with particle embolization · Uncorrectable coagulopathy (in setting of elective cases)
Relative
Severe contrast allergy (premedicate) · Severe renal impairment (limit contrast; use CO₂ adjunct) · Pulmonary artery source (requires PA angiography and coil/plug, not particle embolization)
Pre-Procedure Imaging and Workup
Study
Role
CT angiography (chest)
Identifies hypertrophied bronchial arteries (>2 mm abnormal), ectopic origins, non-bronchial systemic supply, underlying parenchymal disease, pulmonary artery pseudoaneurysm. Standard of care prior to BAE.
Bronchoscopy
Lateralizes bleeding (especially when CT non-localizing), allows airway toilet and protection of non-bleeding side; does not replace CTA for vascular mapping.
Chest radiograph
Initial screen — may show underlying cavity, mass, or infiltrate; non-specific.
Procedure Overview
The following is a high-level summary. Full catheter and microcatheter selection matrices, particle sizing by vessel caliber, sedation protocols, and cone-beam CT parameters are available in RadCall Pro.
Pre-Procedure
Stabilize: airway protection (bleeding-side-down positioning, selective intubation if needed), correct coagulopathy, transfuse if Hgb trending down.
Review CTA: identify culprit vessels, variant/ectopic origins, and non-bronchial systemic collaterals. Lateralize based on parenchymal findings and bronchoscopy.
Consent and anesthesia: moderate sedation is standard; general anesthesia for unstable airway or massive active bleeding.
Access and Diagnostic Angiography
Access: right common femoral artery with 5 Fr sheath; radial access increasingly used.
Descending thoracic aortogram: pigtail catheter at T4–T5 level, AP projection. Survey entire thoracic aorta, subclavians, internal mammaries, and phrenics for culprit and collateral supply.
Selective bronchial artery catheterization: 4–5 Fr Cobra, Mikaelsson, Simmons 1/2, or Shepherd's Hook catheter. Selective injections with gentle hand injection (2–3 mL iodinated contrast); evaluate for hypertrophy, hypervascularity, parenchymal blush, and — critically — spinal branches.
Identifying Abnormal Vessels
Bronchial artery diameter >2 mm is abnormal (normal <1.5 mm).
Tortuosity, hypervascularity, parenchymal blush in region of disease on CT.
Bronchopulmonary shunting (early opacification of pulmonary veins during bronchial injection) indicates large anastomoses; use larger particles (500–700 μm) to avoid systemic embolization.
Extravasation is rarely seen (intermittent bleeding); absence does not rule out the culprit vessel.
Non-bronchial systemic supply must be actively sought — interrogate intercostals (over the pleural abnormality), internal mammary, inferior phrenic, thyrocervical/costocervical trunks.
Embolization
Microcatheter superselection: 2.4–2.8 Fr microcatheter coaxially advanced distal to any spinal branch. Confirm position with hand injection before embolization.
Cone-beam CT (optional but recommended): confirms target territory, identifies occult spinal branches, and detects non-target parenchymal or systemic distribution.
Particle embolization: PVA or tris-acryl gelatin microspheres, 300–700 μm (use 500–700 μm if bronchopulmonary shunting present). Slow, fluoroscopically controlled injection to near-stasis. Avoid reflux.
Endpoint: near-stasis in the culprit vessel with preservation of proximal flow; avoid complete proximal occlusion to allow re-access for recurrence.
Treat all abnormal vessels — bilateral bronchial arteries plus any non-bronchial systemic collaterals. Missing a co-contributing vessel is the leading cause of early rebleeding.
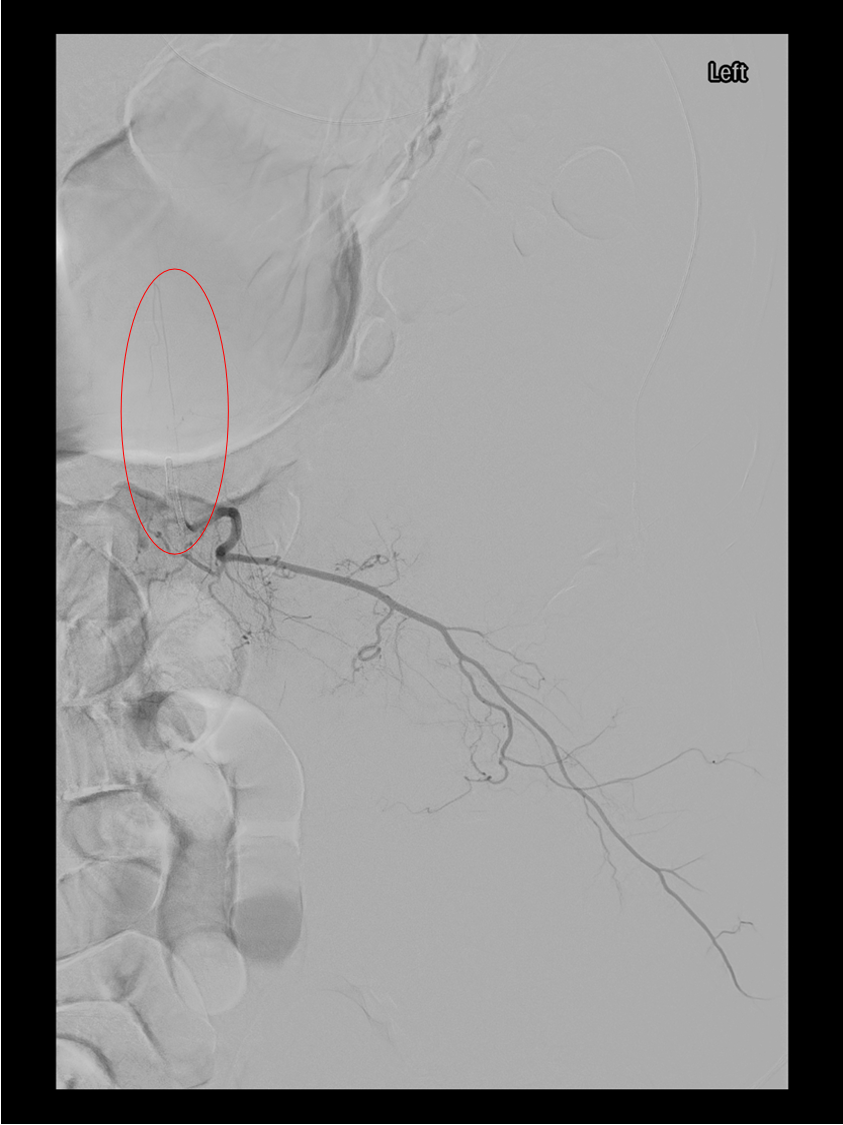
Selective bronchial artery angiogram demonstrating a hypertrophied, tortuous bronchial artery with parenchymal hypervascularity in the territory of disease — the target for particle embolization.
Embolic Agents
Agent
Use
PVA particles 300–500 μm
Standard for most bronchial arteries without bronchopulmonary shunt
PVA particles 500–700 μm
When bronchopulmonary shunting present; reduces risk of paradoxical systemic embolization
Technical success (selective catheterization + embolization of target)
>95%
Causes of Recurrence and Management
Missed non-bronchial systemic supply (most common cause of early failure) — always survey intercostals, IMA, phrenics, thyrocervical/costocervical trunks.
Monitor for recurrent hemoptysis — any recurrence within 30 days warrants repeat imaging and consideration for re-embolization.
Treat underlying disease — antibiotics for infection, antifungals for aspergilloma (often combined with BAE), oncologic therapy for malignancy, CFTR modulators for CF.
Chest CT or CT angiography at 1–3 months if clinical concern for incomplete treatment.
Evidence Summary
Panda A et al (2017) — meta-analysis: immediate clinical success 82–98%; recurrence 10–55% depending on etiology; major complications <1% in modern series.
Yoon W et al (Radiographics 2002, updated 2020s): landmark reviews establishing microcatheter superselection and cone-beam CT as standard; non-bronchial systemic collaterals account for recurrent bleeding in up to 45% of failures.
CIRSE Standards of Practice (2017, CVIR): consensus guidelines on pre-procedure CTA, particle selection, and safety technique.
Flight WG et al (CF hemoptysis series): in CF, BAE is safe and effective but recurrence is frequent; serial embolizations over lifetime are common, and BAE bridges to lung transplantation.
Chun JY et al (CVIR 2010, n=128): cone-beam CT use reduced non-target embolization rate from 10% to 0% and allowed identification of occult spinal branches not seen on 2D angiography.
References
Panda A, Bhalla AS, Goyal A. Bronchial artery embolization in hemoptysis: a systematic review. Diagn Interv Radiol. 2017;23(4):307–317.
Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics. 2002;22(6):1395–1409.
Hartmann IJC, Remy-Jardin M, Menchini L, Teisseire A, Khalil C, Remy J. Ectopic origin of bronchial arteries: assessment with multidetector helical CT angiography. Eur Radiol. 2007;17(8):1943–1953.
Chun JY, Morgan R, Belli AM. Radiological management of hemoptysis: a comprehensive review of diagnostic imaging and bronchial arterial embolization. Cardiovasc Intervent Radiol. 2010;33(2):240–250.
Cauldwell EW, Siekert RG, Lininger RE, Anson BJ. The bronchial arteries: an anatomic study of 150 human cadavers. Surg Gynecol Obstet. 1948;86(4):395–412.
Shin BS, Jeon GS, Lee SA, Park MH. Bronchial artery embolisation for the management of haemoptysis in patients with pulmonary tuberculosis. Int J Tuberc Lung Dis. 2011;15(8):1093–1098.
Sopko DR, Smith TP. Bronchial artery embolization for hemoptysis. Semin Intervent Radiol. 2011;28(1):48–62.
Ittrich H, Bockhorn M, Klose H, Simon M. The diagnosis and treatment of hemoptysis. Dtsch Arztebl Int. 2017;114(21):371–381.
Hwang HG, Lee HS, Choi JS, Seo KH, Kim YH, Na JO. Risk factors influencing rebleeding after bronchial artery embolization on the management of hemoptysis associated with pulmonary tuberculosis. Tuberc Respir Dis. 2013;74(3):111–119.
Kato A, Kudo S, Matsumoto K, et al. Bronchial artery embolization for hemoptysis due to benign diseases: immediate and long-term results. Cardiovasc Intervent Radiol. 2000;23(5):351–357.
Davidson K, Shojaee S. Managing massive hemoptysis. Chest. 2020;157(1):77–88.
Flight WG, Barry PJ, Bright-Thomas RJ, Butterfield S, Ashleigh R, Jones AM. Outcomes following bronchial artery embolisation for haemoptysis in cystic fibrosis. Cardiovasc Intervent Radiol. 2017;40(8):1164–1168.
Full technique in RadCall Pro
Complete catheter and microcatheter matrix, particle sizing algorithm by vessel caliber and shunt pattern, cone-beam CT protocol, and recurrence salvage strategies available in RadCall Pro.