Pulmonary arteriovenous malformations (PAVMs) are right-to-left shunts through an abnormal capillaryless connection between the pulmonary artery and pulmonary vein. Transcatheter embolization of the feeding artery with coils or vascular plugs eliminates the shunt, reverses hypoxemia, and — critically — removes the conduit for paradoxical embolization of venous thrombi and air, which cause stroke and brain abscess in untreated patients.
Key points
HHT is the dominant cause: ~80% of PAVMs occur in hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu); ~50% of HHT patients have PAVMs. The remainder are sporadic.
Treatment threshold: embolize any PAVM with a feeding artery ≥3 mm diameter, regardless of symptoms — paradoxical stroke and brain abscess risk is present even in asymptomatic patients. Emerging evidence supports treating smaller feeders if technically feasible.
Classification: simple PAVM — single segmental feeder; complex PAVM — multiple feeders from two or more segmental arteries (higher recurrence).
Embolic choice: pushable fibered coils, detachable coils, or Amplatzer vascular plugs deployed as close to the sac as possible without occluding normal branches. Plugs preferred for short feeders (large, single device).
Strict air control is mandatory — any air in the catheter system can cross the shunt and cause systemic air embolism (stroke). CO₂ flushing of catheters is contraindicated.
Lifelong CT surveillance at 6–12 months post-procedure and every 3–5 years thereafter — reperfusion occurs in 5–15% via recanalization, missed accessory feeders, or pulmonary–pulmonary collaterals.
Indications and Contraindications
Indication
Notes
PAVM with feeding artery ≥3 mm
Standard threshold (second international HHT guidelines)
Brain MRI: in all HHT patients to screen for cerebral AVMs before pulmonary intervention.
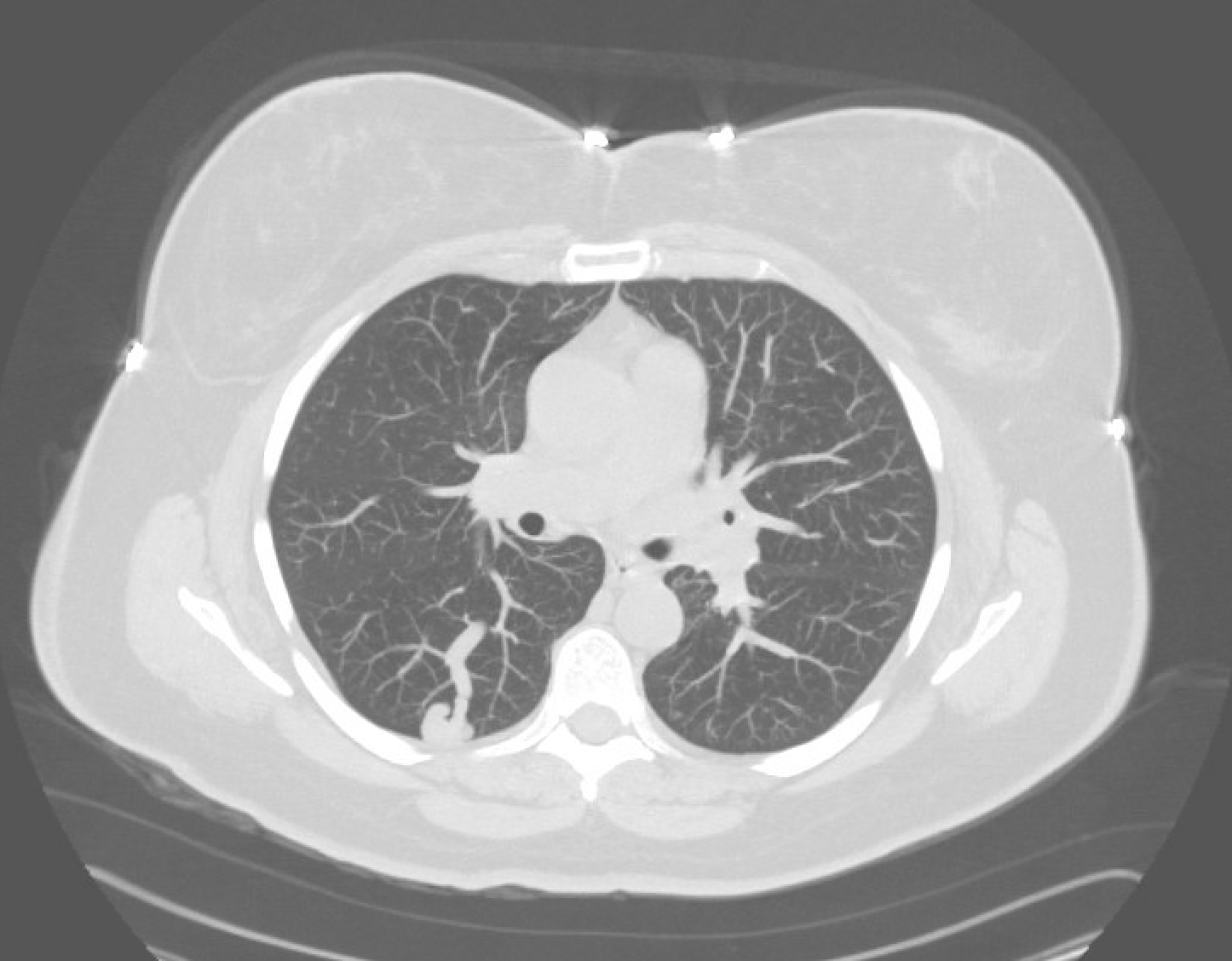
CT chest demonstrating a pulmonary AVM — feeding segmental pulmonary artery, aneurysmal sac, and draining vein to the left atrium.
Air control is paramount. PAVMs are a direct right-to-left conduit. A micro-bubble introduced through the catheter or sheath can cause systemic arterial air embolism and stroke. Aspirate all lines before injection, eliminate bubbles in contrast syringes, and never use CO₂ as a contrast agent or for catheter flushing.
Procedure Overview
The following is a high-level summary. Full catheter and microcatheter matrix, coil sizing algorithm for PAVM feeders, plug selection by feeder length, and reperfusion salvage strategy are available in RadCall Pro.
Pre-Procedure
Pre-procedure CT: map each PAVM, feeding artery diameter, number of feeders, draining vein, and proximity to normal branches.
Baseline SpO₂ supine and upright; shunt fraction if available.
Anticoagulation: heparin during catheterization per operator preference; avoid inadvertent venous thromboembolism in a patient with right-to-left shunt.
Catheterization
Access: right common femoral vein; 7–8 Fr sheath.
Guide catheter: 6–7 Fr guiding sheath or catheter into the main pulmonary artery; selective segmental pulmonary arteriogram (multiple projections) to confirm feeding artery anatomy and count feeders.
Microcatheter selection: advance coaxial microcatheter (2.4–2.8 Fr) into feeding artery as close to the venous sac as possible, distal to any normal branches.
Embolization
Device selection: Amplatzer vascular plug for short, straight, high-flow feeders (single device = efficient occlusion and low reperfusion); detachable or pushable fibered coils for tortuous feeders or when plug oversizing is not feasible.
Sizing: plug diameter 30–50% greater than feeding artery diameter; anchor coil (first coil) oversized by 20–30% of feeder diameter to prevent migration into the sac or pulmonary vein.
Deployment: occlusive device placed at the most distal feeding artery segment; confirm stasis on angiogram before detachment.
Completion angiogram: confirm cessation of flow into sac and persistent perfusion of normal segmental branches. Address any additional feeders before case end.
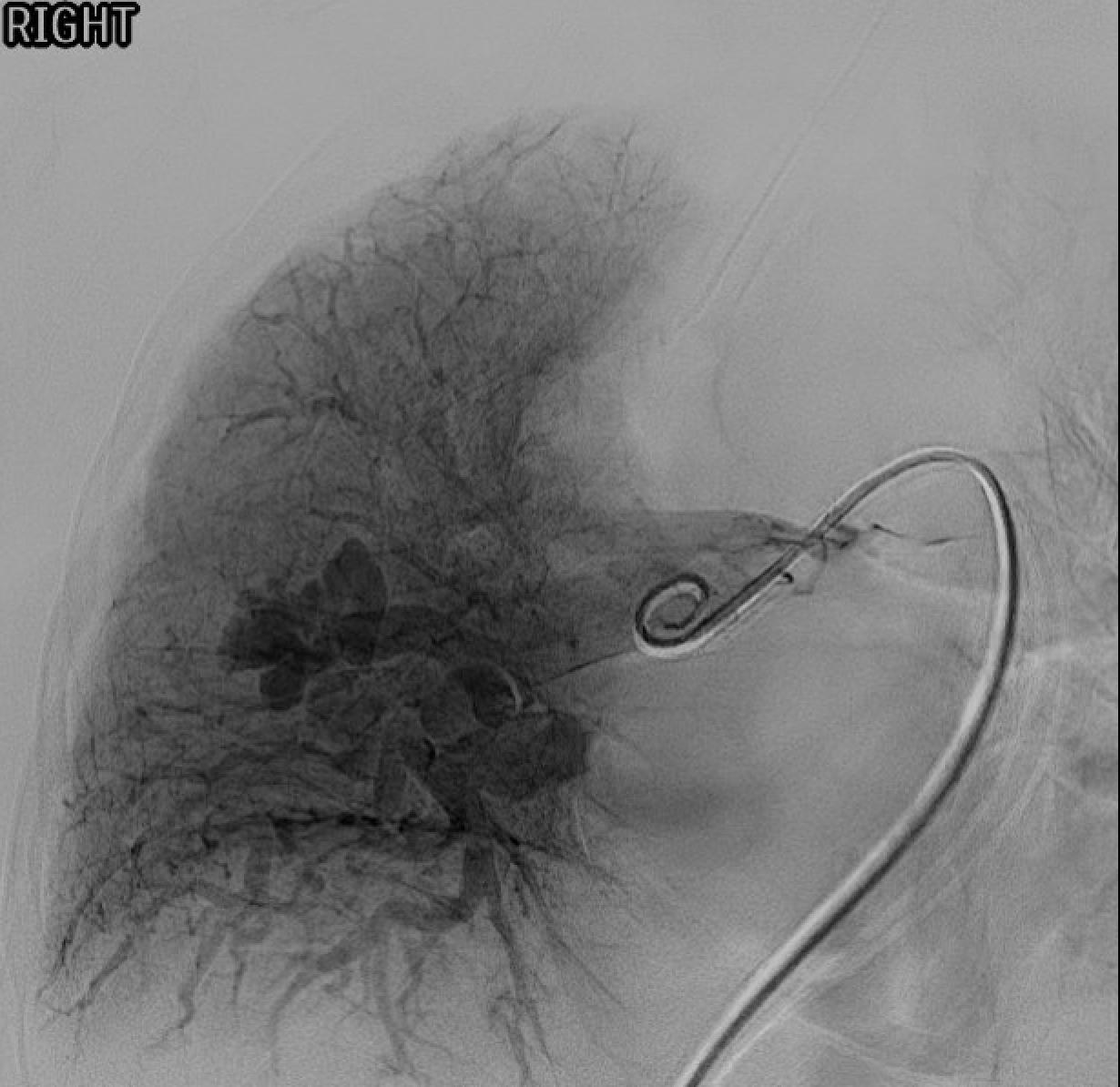
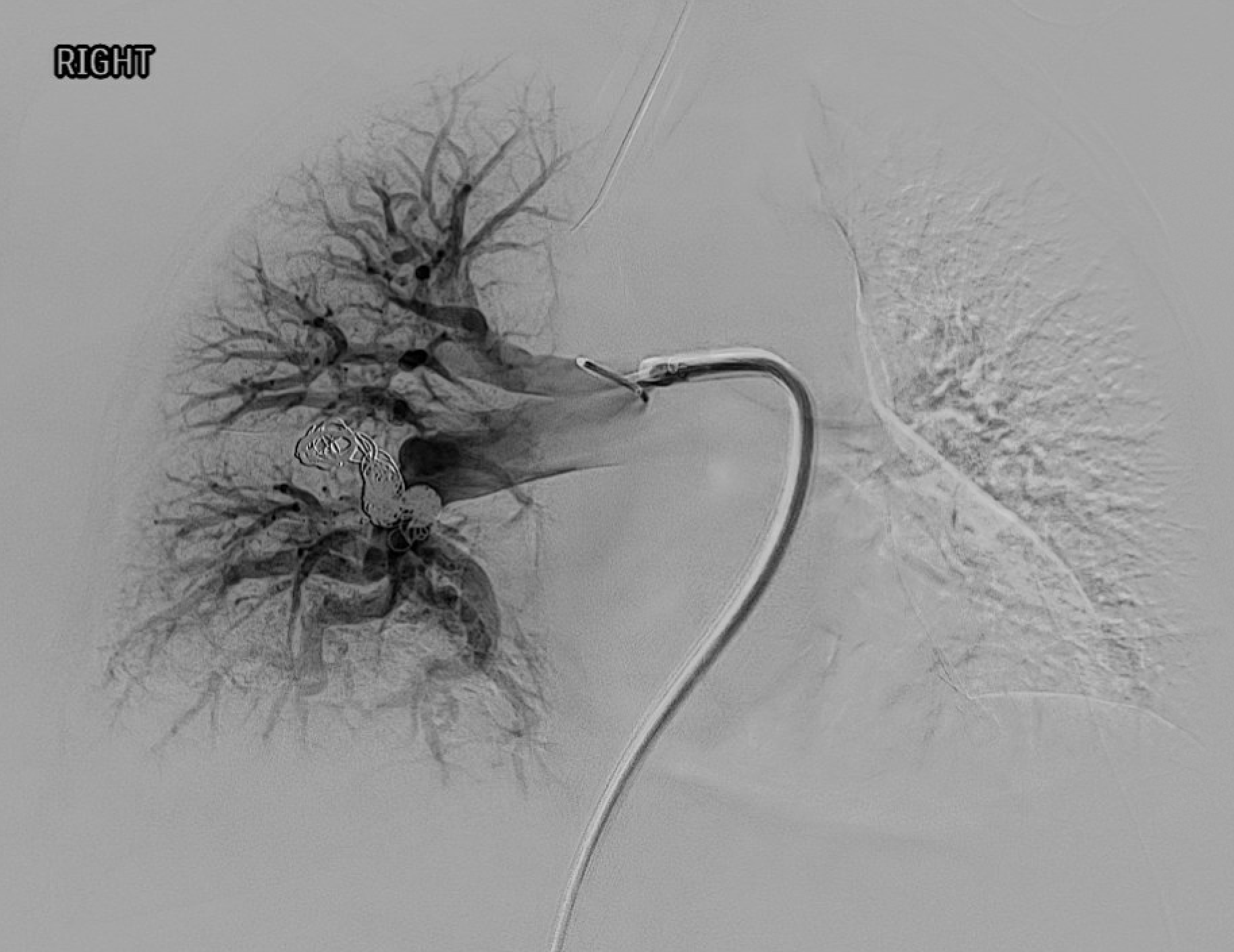
Pre-embolization pulmonary angiogram — contrast filling of the AVM sac via the feeding segmental artery.Post-embolization — coils in the feeding artery with stasis and no residual sac filling on completion angiogram.
Device Selection Summary
Device
Best application
Amplatzer vascular plug (AVP II/IV)
Short straight feeders; single device; faster occlusion; lower reperfusion than coils alone
Detachable coils
Tortuous or distal feeders; controlled release; precise placement
Pushable fibered coils
Inexpensive; larger-volume occlusion; risk of malposition if not oversized
MicroVascular Plug (MVP)
Small feeders (3–7 mm); low-profile 2.4 Fr delivery through microcatheter
Complications
Complication
Rate
Management
Pleuritic chest pain / pleurisy
10–30%
Self-limited; NSAIDs; more common with larger PAVMs and near-pleural sacs
Paradoxical air embolism (angina, stroke, TIA)
<1%
Preventable with strict air control; 100% oxygen, supportive care if occurs; almost always transient
Device migration to pulmonary vein / systemic circulation
<1%
Catastrophic if systemic; prevented by proper oversizing; snare retrieval if caught early
Recanalization / reperfusion
5–15% (higher for coils than plugs; higher for complex PAVM)
Re-embolization at follow-up
Infarction / pulmonary hemorrhage
Rare
Usually self-limited
Contrast reaction / nephropathy
Low
Premedicate allergic; hydrate
Post-Procedure Care and Surveillance
Observation: overnight admission is typical; many centers now discharge same day for uncomplicated single-PAVM cases.
Antibiotic prophylaxis: lifelong antibiotic prophylaxis for dental and invasive procedures in HHT with PAVM history — brain abscess risk persists even after embolization due to reperfusion or missed PAVMs.
CT surveillance: thin-section chest CT at 6–12 months post-procedure; then every 3 years if stable; lifelong follow-up given reperfusion and new-AVM risk.
Criteria for sac resolution: ≥70% reduction in sac diameter or complete disappearance indicates successful occlusion; persistent sac enhancement or enlargement suggests reperfusion.
Re-screening: repeat contrast echocardiography in persistent shunt or before pregnancy.
Genetic counseling and family screening for HHT patients.
Evidence Summary
Faughnan ME et al (2020, Second International HHT Guidelines, Ann Intern Med): embolize all PAVMs with feeding artery ≥3 mm; treat smaller feeders if technically feasible; lifelong CT surveillance.
Pollak JS et al (2006, J Vasc Interv Radiol): long-term series showing Amplatzer plug superior to coils for reducing reperfusion.
Andersen PE & Kjeldsen AD (2010): long-term follow-up of PAVM embolization; reperfusion 5–15%, mostly amenable to re-embolization.
Trerotola SO & Pyeritz RE (2010, AJR): review of PAVM diagnosis and management including the 3-mm feeder threshold — now being revisited downward as smaller feeders carry measurable paradoxical-embolism risk.
References
Faughnan ME, Mager JJ, Hetts SW, et al. Second international guidelines for the diagnosis and management of hereditary hemorrhagic telangiectasia. Ann Intern Med. 2020;173(12):989–1001.
Pollak JS, Saluja S, Thabet A, Henderson KJ, Denbow N, White RI Jr. Clinical and anatomic outcomes after embolotherapy of pulmonary arteriovenous malformations. J Vasc Interv Radiol. 2006;17(1):35–45.
Trerotola SO, Pyeritz RE. PAVM embolization: an update. AJR. 2010;195(4):837–845.
Shovlin CL. Pulmonary arteriovenous malformations. Am J Respir Crit Care Med. 2014;190(11):1217–1228.
Andersen PE, Kjeldsen AD. Clinical and radiological long-term follow-up after embolization of pulmonary arteriovenous malformations. Cardiovasc Intervent Radiol. 2010;33(4):844–851.
Hsu CCT, Kwan GNC, Thompson SA, Evans-Barns H, van Driel ML. Embolisation for pulmonary arteriovenous malformation. Cochrane Database Syst Rev. 2018;1:CD008017.
Shovlin CL, Guttmacher AE, Buscarini E, et al. Diagnostic criteria for hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome). Am J Med Genet. 2000;91(1):66–67.
Full technique in RadCall Pro
Complete catheter and microcatheter matrix, coil sizing algorithm, Amplatzer plug selection by feeder length and diameter, and reperfusion salvage strategies available in RadCall Pro.