Anatomy and Fracture Regions
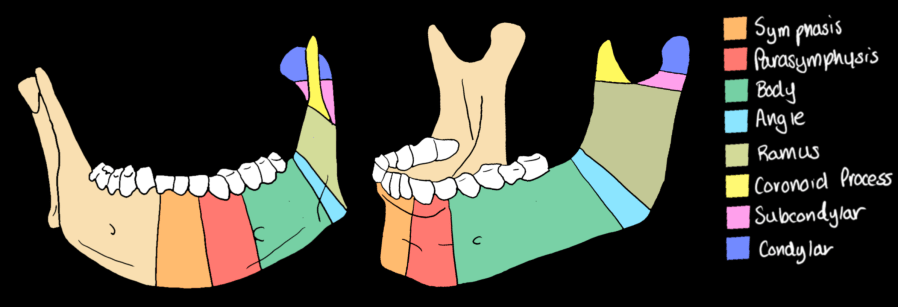
The mandible is classified into seven anatomic regions. Because of its ring structure, isolated single fractures are uncommon — two fractures at different sites are typical after blunt trauma.
| Region | Location | Key Points |
|---|---|---|
| Symphysis | Midline, between the two central incisors | Parasymphyseal fractures extend from canine to canine; both are tooth-bearing |
| Body | Posterior to parasymphysis through the mental foramen to the anterior border of the masseter | Tooth-bearing; fractures here invariably traverse the inferior alveolar canal |
| Angle | Third molar region at the junction of body and ramus | Most common site (~36%); impacted third molar weakens the angle; highest postoperative complication rate |
| Ramus | Vertical strut from angle to condylar neck | Thick bone; protected by masseter; rarely fractured in isolation |
| Condyle | Articulates with the glenoid fossa; subdivided into intracapsular (condylar head) and subcondylar (condylar neck/base) | Intracapsular = avascular necrosis and TMJ ankylosis risk; subcondylar = most amenable to ORIF |
| Coronoid process | Anterior ramus; within infratemporal fossa | Rare; associated with depressed zygomatic arch fractures |
| Alveolar process | Tooth-bearing ridge; separate from body fractures | Usually treated conservatively |
Fracture Classification
Tooth-bearing vs. non-tooth-bearing: Fractures through the tooth-bearing region (symphysis, parasymphysis, body, angle) communicate with the oral cavity through the periodontal ligament — these are compound fractures and carry infection risk. The only exception is an unerupted third molar with no gingival tear.
Comminuted fractures: Defined as >3 fragments within the same anatomic region. The full length of the comminuted segment must be described — inadequate plate length (fewer than 3 screws on each side of the bridged segment) is a common cause of hardware failure.
Flail mandible: Trifocal fractures (parasymphyseal + bilateral condylar) or bilateral angle/body fractures create an unstable free anterior segment. Loss of genioglossus attachment risks glossoptosis and airway compromise — flag explicitly for the trauma team.
All fractures of the tooth-bearing mandible are compound by definition (they communicate with the oral cavity via the periodontal ligament). Soft-tissue gas on CT confirms compound nature. Tooth fractures and avulsed teeth should be reported — ingested or aspirated teeth require evaluation of the aerodigestive tract.
Key Preoperative CT Findings
| Finding | What to Report | Clinical Significance |
|---|---|---|
| Inferior alveolar canal | Fracture line crossing the canal; displacement >5 mm | Higher risk of inferior alveolar nerve injury; surgical planning |
| Comminution | Number of fragments; full craniocaudal and anteroposterior extent | Dictates plate length (≥3 screws on each side of bridged segment required) |
| Lingual cortex | Lingual gap (posteriorly divergent fracture) on axial images | If missed, results in lingual malreduction and facial widening |
| Basal triangles | Butterfly fractures; inferior basal fragments | Risk of fragment displacement and hardware failure |
| Flail mandible | Trifocal (parasymphyseal + bicondylar); bilateral angle; bilateral body | Airway compromise risk; glossoptosis; emergent alert |
| Tooth extraction indicators | Gross periodontal disease, large caries, root fracture in fracture line | May favor early extraction to reduce infection risk |
| Edentulous atrophic mandible | Measure vertical body height (see Luhr classification below) | Determines nonunion risk and fixation strategy |
Luhr Classification — Edentulous Atrophic Mandible:
| Class | Mandibular Body Height | Nonunion Risk |
|---|---|---|
| I | 16–20 mm | Lowest |
| II | 11–15 mm | Intermediate |
| III | ≤10 mm | Highest — inadequate bone cross-section for standard fixation |
Condylar and Subcondylar Fractures
Condylar fractures are the second most common mandibular fracture site. Most are treated with closed reduction (mandibulomaxillary fixation, MMF), but ORIF is increasingly used.
Subcondylar ORIF indicators (report explicitly):
| Finding | Threshold |
|---|---|
| Ramus shortening | >15 mm |
| Condylar head angulation | >35° |
| Posterior vertical height loss | Bilateral (anterior open bite on 3D) |
| Bone contact between ramus and zygomatic arch | Any (prevents reduction) |
| Intracapsular condylar head fracture | High ORIF risk; avascular necrosis risk |
TMJ ankylosis (late complication): Traumatic displacement of the articular disk is the most important predictor. On CT: heterotopic bone between condylar head and glenoid fossa/zygomatic arch on coronal images. MRI is the only reliable noninvasive tool for direct disk evaluation in the acute setting.
Postoperative CT Findings
| Finding | Imaging Features | Significance |
|---|---|---|
| Adequate reduction | No lingual gap on axial CT; restored lower facial width on 3D | Goal of ORIF |
| Lingual gap | Posteriorly divergent fracture gap on axial images | Malreduction; causes facial widening; requires revision |
| Nonunion | Persistent fracture line >8 weeks; no bridging trabeculation | Leads to hardware failure and osteomyelitis |
| Osteomyelitis | Irregular resorbed bone, mottled or rounded sclerotic edges, sequestration of devitalized fragments | Major complication; requires debridement ± staged reconstruction |
| Hardware failure | Plate fracture, bending, loosening, or migration | Before osseous union = major complication (requires repeat osteosynthesis); after union = minor complication |
| Abscess / fistula | Low-attenuation collection with peripheral enhancement adjacent to hardware or fracture site | Submandibular or neck abscess requires incision, drainage, and IV antibiotics |
Osseous union normally occurs within 8 weeks. Hardware failure before union requires repeat osteosynthesis. After union is established, loose or infected hardware can often be removed in an office procedure. Screws within 10 mm of infected bone carry higher failure risk — note proximity to involved segments.
Reporting Checklist — Mandibular Fractures
Preoperative:
- Fracture location(s): symphysis / parasymphysis / body / angle / ramus / condyle / coronoid / alveolar
- Fracture line and inferior alveolar canal: crossing present / absent; displacement (mm) at canal
- Comminution: present / absent; number of fragments; full extent of comminuted segment
- Lingual cortex: intact / lingual gap present (describe location)
- Basal triangles / butterfly fragments: present / absent
- Flail mandible pattern: alert if trifocal, bilateral angle, or bilateral body
- Tooth-related findings: periodontal disease / caries / root fracture in fracture line
- Edentulous mandible: measure mandibular body height; Luhr class I / II / III
- Condyle: intracapsular / subcondylar; ramus shortening (mm); angulation (degrees); bone contact with zygomatic arch
- Airway: sublingual/submandibular hematoma; glossoptosis risk; soft-tissue gas
- Teeth: avulsed / fractured crowns; radiolucent socket (acute tooth loss)
Postoperative:
- Reduction adequacy: lingual gap present / absent; facial width on 3D images
- Osseous union: bridging trabeculation present / absent; fracture line status at 8 weeks
- Osteomyelitis: irregular resorbed bone / sclerotic edges / sequestration / mottled appearance
- Hardware: intact / fractured / bent / loose / migrated; proximity to infected bone
- Abscess / fistula: location; sinus tract to skin
- Condylar healing: TMJ ankylosis — heterotopic bone / fibrous / normal
Reference
Dreizin D, Nam AJ, Diaconu SC, Bernstein MP, Bodanapally UK, Munera F. Multidetector CT of Mandibular Fractures, Reductions, and Complications. RadioGraphics. 2016;36(5):1539–1564.