Classic presentation: Bilious vomiting in a neonate. Any neonate with bilious vomiting requires urgent imaging to exclude volvulus. Older children may present with chronic, intermittent abdominal pain, vomiting, weight loss, or failure to thrive.
Malrotation vs. Nonrotation
| Type | DJJ Position | Cecum | Mesenteric Root | Volvulus Risk |
|---|---|---|---|---|
| Normal rotation | Left of midline, at level of duodenal bulb; anchored by ligament of Treitz | Right lower quadrant; fixed by Ladd bands | Wide | Low |
| Malrotation | Right of midline or midline; not at level of duodenal bulb | Usually right upper quadrant (high) | Narrow | High |
| Nonrotation | Midline or right | Midline or left hemiabdomen; all small bowel right-sided | Wide | Low (late presentation) |
Midgut volvulus is a surgical emergency. The narrow mesenteric root in malrotation allows the entire midgut to twist around the SMA, causing bowel ischemia within hours. Mortality/morbidity 3–5%, increasing significantly with delayed diagnosis and treatment. Do not wait for additional imaging if volvulus is confirmed — emergent surgical consultation immediately.
Imaging Approach
Ultrasound is now recommended as the first-line study — faster, no radiation, bedside-capable. UGI fluoroscopy remains the diagnostic reference standard and should follow immediately if US is inconclusive.
| Modality | Role |
|---|---|
| Abdominal radiograph | Usually nonspecific; may show double bubble, paucity of bowel gas, or proximal obstruction; does not exclude malrotation |
| Ultrasound | First-line; assess SMA/SMV relationship and D3 position; whirlpool sign for volvulus |
| UGI fluoroscopy | Reference standard; definitively assesses DJJ position and duodenal course |
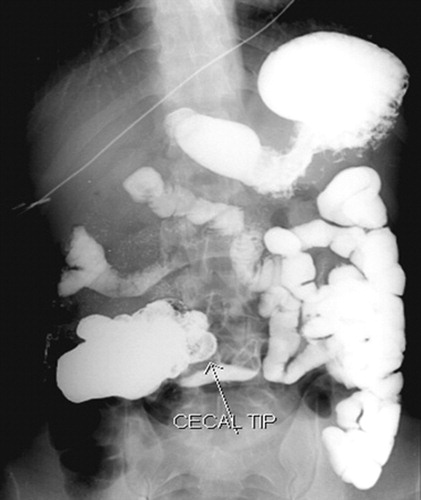
| Lower GI contrast | Performed when UGI is equivocal; demonstrates cecal position |
| CT | Not routine; used in older children with unclear chronic presentation |
Ultrasound
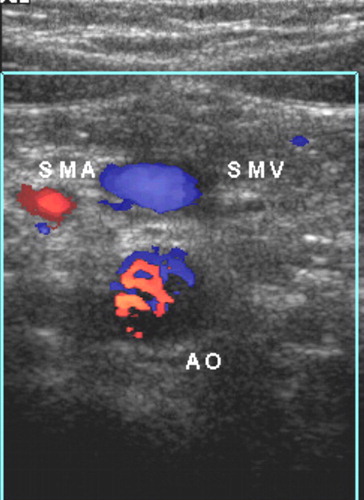
SMA/SMV Relationship
The SMV normally lies to the right of the SMA (evaluate relative to the SMA–aorta axis — draw a line through the SMA and aorta; SMV should be on the right of this line).
| Finding | Significance |
|---|---|
| SMV right of SMA | Normal — but present in 29% of malrotation cases (insufficient to exclude) |
| SMV left of SMA | Abnormal — seen in 47% of malrotation cases |
| SMV aligned with SMA | Indeterminate — seen in 24% of malrotation cases |
SMA/SMV relationship alone is unreliable. It is normal in nearly a third of malrotation cases. The more sensitive and specific sign is the position of the third part of the duodenum (D3).
D3 Position (More Sensitive)
The D3 normally takes a retroperitoneal course posterior to the SMA, crossing the midline between the aorta and SMA at the level of the uncinate process of the pancreas.
- Normal: D3 seen posterior to the SMA, crossing midline in a retroperitoneal position
- Abnormal: D3 courses anteriorly (intraperitoneal), fails to cross midline posterior to SMA
Technique: 12–18 MHz transducer; graded compression; sweep cranial to caudal from the epigastrium; identify SMA, SMV, and aorta before looking for D3. Smaller microconvex probe helps in smaller infants.
Pitfall: Jejunal loops crossing the midline below the uncinate process of the pancreas can mimic D3. D3 is the only small bowel segment with a true retroperitoneal course — identify it above the level where jejunum crosses.
Whirlpool Sign (Volvulus)
Clockwise swirling of the SMV and its branches around the SMA while scanning cranially to caudally = midgut volvulus. Additional findings:
- Thickening of the twisted midgut
- Dilatation of D2 proximal to the twist
- Engorgement of mesenteric vessels; narrowing of SMA at the center of the whirlpool
Clockwise vs. anticlockwise: An anticlockwise whirlpool of a branch of the SMV around the SMA without bowel involvement is a normal variant — do not mistake for volvulus. True volvulus: clockwise rotation, bowel loops incorporated in the whirl, Doppler confirms vascular compromise. Use real-time scanning and cine images to differentiate.
UGI Fluoroscopy
Technique: Position infant right-side down in true lateral; inject contrast via nasogastric tube (preferred in acute setting for volume control and aspiration prevention; ~10–20 mL); document duodenal sweep in both lateral and AP views.
Four Criteria for Normal Rotation (All Must Be Met)
| Criterion | Normal Finding |
|---|---|
| 1. Retroperitoneal duodenum | D2 and D4 nearly superimposed on true lateral view |
| 2. DJJ left of left vertebral pedicle | DJJ lies to the left of the left pedicle of L1–L2 on AP view |
| 3. DJJ at level of duodenal bulb | DJJ at the same height as the duodenal bulb on AP view |
| 4. Proximal jejunum in left upper quadrant | First jejunal loops course into the left upper abdomen |
Fluoroscopic Signs of Midgut Volvulus
| Sign | Description |
|---|---|
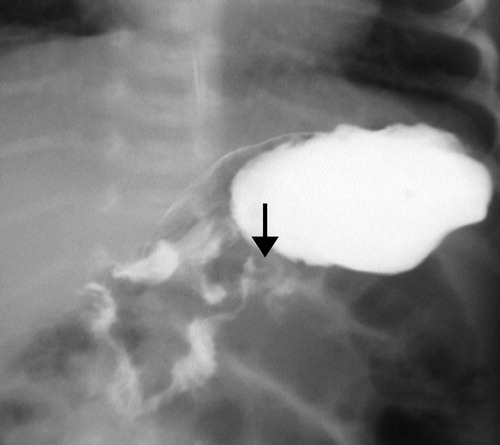
| Corkscrew sign | Spiral/twisting course of D3 and proximal jejunum — most classic sign |
| Beaking | Transitional tapering between D2 and D3; partial or complete obstruction |
| Proximal dilatation | Dilation of the duodenal bulb and D2 with hold-up of contrast |
| DJJ right of midline | Abnormal; proximal small bowel loops to the right of midline |
Corkscrew sign may only be visible on one view. Always assess the duodenum on both frontal and lateral projections before concluding the study is normal. In partial volvulus, contrast may pass with a minimal twist — subtle beaking or rightward DJJ position may be the only clue.
Pitfalls on UGI:
- Duodenum inversum — rare normal variant where D3 crosses right then courses left above the pancreas; can simulate malrotation
- Inferior DJJ displacement — splenomegaly, overdistended stomach, or transplanted left liver segment can push DJJ inferiorly → false positive
- Peritoneal ligamentous laxity — DJJ is mobile in infants; verify position on multiple frames
Fluoroscopic Images

Whirlpool Sign Mimics
| Pattern | Direction | Bowel Involved | Significance |
|---|---|---|---|
| Midgut volvulus | Clockwise | Yes | Surgical emergency |
| Normal SMV branch variant | Anticlockwise | No | Normal variant — do not treat |
| Intussusception target sign | Concentric rings (not a whirl) | Yes | Enema reduction |
Key distinguishing tip: Identify the terminal ileum and cecum in every patient. Normal terminal ileum and cecum without bowel wall thickening argues against ileocolic intussusception and toward volvulus when a circular RUQ lesion is present.
Associated Anomalies
Malrotation may be isolated or associated with:
- Situs ambiguus / heterotaxy — 70% of heterotaxy patients have malrotation
- Duodenal atresia, intestinal atresia, Hirschsprung disease
- Biliary atresia, choledochal cyst
- Congenital diaphragmatic hernia
- Omphalocele, gastroschisis
- Chromosomal anomalies (trisomy 13, 18, 21)
- Congenital heart disease
Left-sided appendix on any imaging study should prompt evaluation for underlying intestinal rotation abnormality.
Management — Ladd Procedure
The only definitive treatment for malrotation (elective) and midgut volvulus (emergency). Steps:
- Detorsion of volvulus (if present)
- Division of Ladd bands
- Broadening of the mesenteric root
- Placement of bowel in nonrotation position (small bowel right, large bowel left)
- Appendectomy (to prevent diagnostic confusion with future appendicitis in an ectopic position)
Recurrent volvulus after Ladd procedure: Rare (2–7%) — caused by re-narrowing of the mesenteric root by new adhesions. Consider in any post-Ladd patient presenting with bilious vomiting.