Talus — Hawkins-Canale Classification (Neck)
Talar neck fractures carry high risk of avascular necrosis due to the tenuous blood supply of the talus. The Hawkins-Canale classification stratifies AVN risk by degree of displacement and associated dislocation.
| Type | Description | AVN Risk |
|---|---|---|
| I | Nondisplaced neck fracture | ~10% |
| II | Neck fracture + subtalar dislocation | ~30% |
| III | Neck fracture + tibiotalar dislocation | >90% |
| IV | Neck fracture + talonavicular dislocation | >90% |
Hawkins Sign: A subchondral lucent band at the talar dome seen 4–9 weeks after injury indicates revascularization — osteonecrosis will not develop. Absence of the Hawkins sign raises concern for AVN.
Sneppen Classification (Talar Body)
| Type | Description |
|---|---|
| A | Dome compression |
| B | Coronal shear |
| C | Sagittal shear |
| D | Posterior tubercle fracture |
| E | Lateral tubercle fracture |
| F | Crush |
Special Talar Fractures
Shepherd fracture: Posterior process fracture — mimics os trigonum on imaging. Correlate with clinical history.
Cedell fracture: Posteromedial tubercle fracture — uncommon and easily missed.
Lateral process fracture ("Snowboarder's fracture"): Easily missed on radiograph; CT is required. Should be sought in snowboarders and after ankle inversion injuries.
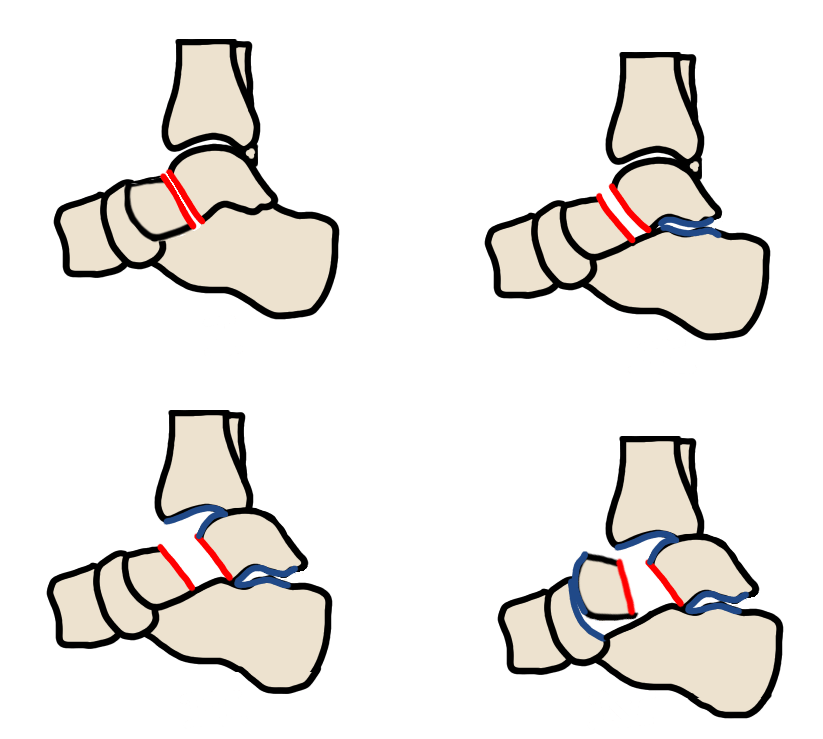
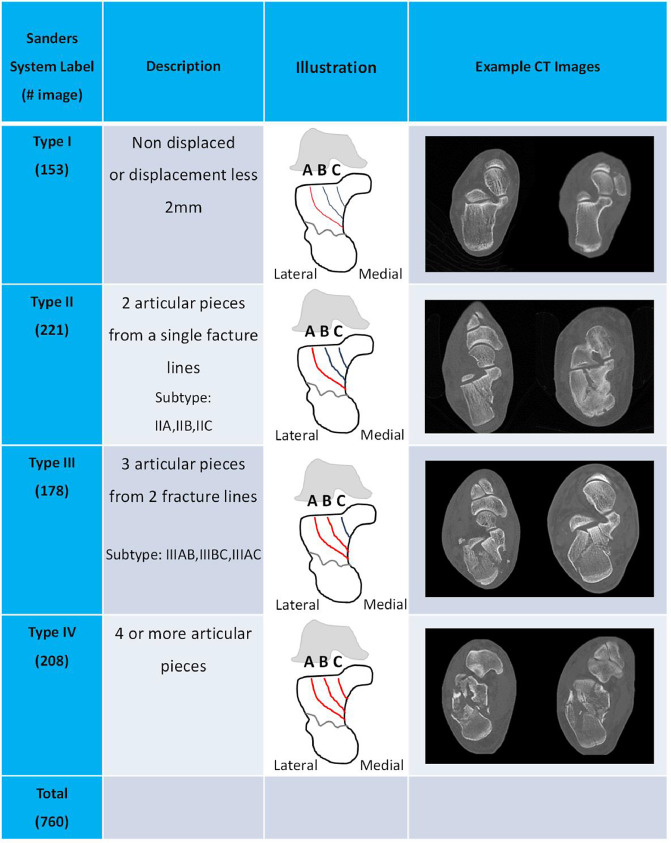
Calcaneus — Sanders Classification (CT-based)
The Sanders classification uses a coronal CT cut through the widest portion of the posterior facet of the subtalar joint. The location of primary fracture lines within the posterior facet determines type.
| Type | Description |
|---|---|
| I | Nondisplaced (regardless of number of fragments) |
| II | Two-part posterior facet — subdivided A, B, C from lateral to medial |
| III | Three-part — two fracture lines in the posterior facet |
| IV | Four or more fragments (comminuted) — primary subtalar arthrodesis often preferred |
Reporting Checklist — Calcaneus
- Number of sagittal lines entering the posterior subtalar joint
- Degree of articular fragment depression
- Cortical fragments between dominant fragments (impede reduction)
- Extension into the calcaneocuboid joint
- Peroneal retinaculum avulsion
- Peroneal tendon entrapment
- Fragments inferior to the sustentaculum tali — FHL tendon or tibial nerve entrapment
Lisfranc Injury (Tarsometatarsal)
Lisfranc injuries range from purely ligamentous sprains to high-energy fracture-dislocations. The second metatarsal base is the key to evaluation.
Low-energy (sprain):
- Lateral or dorsal displacement of the second metatarsal on the second cuneiform (most reliable finding)
- Greater than 2 mm first to second metatarsal diastasis on weight-bearing AP view
- Fleck sign — avulsion fracture at the second metatarsal base; pathognomonic for Lisfranc ligament avulsion
High-energy (fracture-dislocation):
- Homolateral — all metatarsals displaced laterally
- Divergent — first metatarsal medial, second through fifth lateral
- Isolated — single metatarsal involvement
Forefoot
Jones fracture: Transverse fracture at the proximal fifth metatarsal diaphysis, approximately 1.5 cm from the base. Prone to nonunion due to tenuous vascularity at the metaphyseal-diaphyseal junction. Treated with intramedullary screw in athletes.
Pseudo-Jones / Dancer's fracture: Avulsion of the peroneus brevis at the fifth metatarsal styloid base. Usually heals conservatively. Not a Jones fracture.
Freiberg disease: Osteochondrosis of the metatarsal head, most commonly the second metatarsal. Occurs in adolescent females. Radiographs show flattening and fragmentation of the metatarsal head.
Turf toe: First MTP plantar plate injury from hyperextension mechanism. MRI is the imaging modality of choice.
Mueller-Weiss syndrome: Adult navicular avascular necrosis with medial collapse and fragmentation.
Reporting Cautions
- Phalangeal tuft fracture: Correlate clinically for nailbed injury, which would make this an open fracture.
- Isolated lesser trochanter avulsion in adults: Consider underlying malignancy and pathologic fracture.
Reference
Siddiqui NA et al. Tarsometatarsal joint evaluation. RadioGraphics. 2014;34(2):514–531.