Fluoroscopic arthrography uses direct intra-articular contrast injection to confirm needle placement before MR arthrogram or to provide diagnostic information about joint integrity. The fluoroscopic component confirms intra-articular position; MRI or CT provides the primary diagnostic images.
Indications
MR arthrogram preparation: Joint injection to distend the capsule and improve detection of internal derangement (labral tears, ligamentous injury, loose bodies)
Therapeutic injection confirmation: Corticosteroid or anesthetic injected under fluoroscopy for confirmed intra-articular delivery
Contraindications
Contraindication
Notes
Active joint septic arthritis
Aspiration for culture is indicated; do NOT inject contrast or gadolinium
Allergy to iodinated contrast
Use alternative approach (MRI without arthrogram, US-guided)
Overlying cellulitis or skin infection
Avoid injection through infected tissue
Coagulopathy
Relative; discuss with referring physician; aspirin/NSAIDs generally held 5 days
Joint-Specific Access and Injection Protocol
MR arthrogram mixture (all joints): 0.1 mM/mL gadolinium — practical recipe per 14 mL: 0.1 mL gadolinium (e.g., gadobutrol or gadopentetate) + 0.5 mL Omnipaque 300 + 13.4 mL normal saline. The Omnipaque allows fluoroscopic visualization of the injectate.
Needle: 22-gauge spinal needle for all joints. Confirm intra-articular position with 0.5–1 mL Omnipaque 300 before injecting the full arthrogram volume.
Junction of medial femoral neck and head; avoid femoral neurovascular bundle medially
12–14 mL
Wrist
Dorsal radiocarpal
Scapholunate interval or radioscaphoid joint; 3–4 cm distal to Lister's tubercle
3–4 mL
Ankle
Anteromedial or anterolateral
Talar dome; tibiotalar joint space
8–10 mL
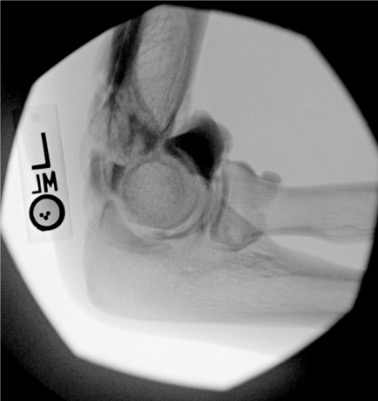
Elbow
Posterior (olecranon fossa)
Olecranon fossa with elbow flexed 90°; needle directed anteriorly into trochlear notch
8–10 mL
Knee
Lateral subpatellar or medial
Subpatellar fat pad; suprapatellar for aspiration of effusion
30–40 mL
Wrist injected volume is small. The radiocarpal compartment holds only 3–4 mL — resistance is felt quickly. Stop injecting if resistance increases before target volume; overdistension causes capsular rupture and contrast extravasation that can obscure compartment communication findings.
Joint Images — Needle Placement and Post-Injection
Intra-articular vs. extra-articular contrast distribution is the key fluoroscopic finding. Intra-articular: contrast flows freely along articular cartilage, fills joint recesses and capsular attachments. Extra-articular: contrast pools in soft tissue planes without joint recess filling — reposition needle before injecting diagnostic volume.
Pattern
Interpretation
Free flow along articular cartilage; fills joint recesses
Intra-articular — proceed with full injection
Soft tissue pooling; irregular tracks in fascial planes
Extra-articular — reposition
Resistance to injection
Extra-articular or needle tip against cartilage/bone — withdraw slightly
Contrast flows into bursa
Bursal communication (rotator cuff full-thickness tear if subacromial; TFCC tear if DRUJ communicates with radiocarpal)
Key Diagnostic Findings
Shoulder
Finding
Fluoroscopic Appearance
Full-thickness rotator cuff tear
Contrast fills the subacromial/subdeltoid bursa = communication with glenohumeral joint through full-thickness tear
Biceps tendon sheath filling
Normal — the long head biceps tendon sheath communicates with the glenohumeral joint
Capsular adhesion (frozen shoulder)
Reduced joint volume; capsule does not distend; obliteration of axillary and subscapularis recesses
Labral tear (SLAP/Bankart)
Not diagnosed on fluoroscopy — MR arthrogram images are diagnostic
Wrist
Finding
Fluoroscopic Appearance
TFCC tear
Contrast from radiocarpal joint fills the distal radioulnar joint (DRUJ)
Scapholunate ligament tear
Contrast from radiocarpal joint fills the midcarpal compartment through the scapholunate interval
Lunotriquetral ligament tear
Contrast fills midcarpal from radiocarpal through lunotriquetral interval
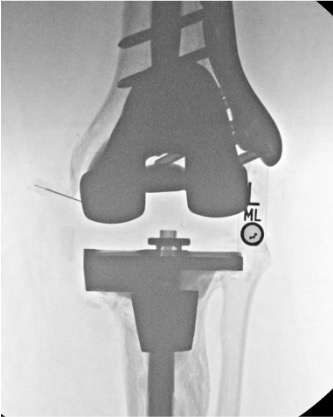
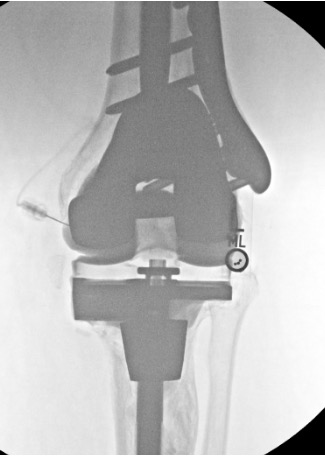
Post-Arthroplasty
Finding
Significance
Contrast tracking along prosthesis-bone interface
Loosening (confirm with delayed fluoroscopy; contrast should clear in intact prosthesis)
Fistulous tract to adjacent soft tissue
Periprosthetic infection — aspirate joint fluid for culture before injecting contrast
Communication with adjacent joint or bursa
Erosion of joint capsule
Post-arthroplasty arthrogram uses iodinated contrast only — no gadolinium. Joint aspiration should precede contrast injection when infection is suspected; send fluid for cell count, Gram stain, culture, and crystal analysis.
Reporting Checklist
Joint accessed: (name, approach)
Needle: 22-gauge spinal
Intra-articular confirmation: confirmed by free contrast distribution / soft tissue injection (if occurred, note and document repositioning)
Omnipaque 300 test dose: volume used (mL)
Total arthrogram volume injected: (mL) — gadolinium/Omnipaque/saline mixture
Bursal communication (shoulder): absent / present (subacromial = full-thickness RCT)
Compartment communication (wrist): absent / present (DRUJ = TFCC; midcarpal = SL or LT)
Patient transferred to MRI / CT for arthrogram sequences
Common Pitfalls
Pitfall
How to Avoid
Extra-articular injection
Use small test dose (0.5–1 mL) under fluoroscopy before injecting full volume; confirm distribution pattern before proceeding
Shoulder: missing subacromial bursal fill
If evaluating for RCT by arthrogram, upright positioning after injection shows bursal fill better; take fluoroscopic images in multiple positions
Gadolinium overdose
Standard MR arthrogram concentration is 0.1 mM/mL (highly diluted) — do not inject undiluted gadolinium intra-articularly; causes synovitis and cartilage damage
Post-arthroplasty: contrast in cement mantle mistaken for loosening
Cement mantle may have defects that fill with contrast without true loosening; compare with prior films; delayed imaging (15 min) helps distinguish true interface tracking from cement defects
Wrist: wrong compartment
Wrist has three compartments (radiocarpal, midcarpal, DRUJ) — each must be entered separately for complete three-compartment arthrogram if indicated; inadvertent midcarpal entry misses radiocarpal pathology
Step-by-step fluoroscopy technique and systematic search patterns available in RadCall Pro.
More in RadCall
99+ guides, IR procedure playbooks, systematic search patterns, case logging, and wRVU tracking — all in one place.