Segments I–VIII based on hepatic veins (divide segments) and portal veins (divide right vs left). Functional right lobe: V–VIII. Functional left lobe: I–IV. Right hepatic vein: divides VI/VII from V/VIII. Middle hepatic vein: true lobar fissure (with gallbladder fossa).
Foley catheter position: within bladder / malpositioned / not present
Urethral Injuries
Type I — Stretch/elongation, no extravasation · Type II — Partial disruption above UGD · Type III — Complete disruption above UGD (most common posterior injury) · Type IV — Bladder neck injury · Type V — Partial/complete anterior urethral injury
Retrograde urethrogram required to evaluate for urethral injury before catheter placement in pelvic fracture with blood at urethral meatus, perineal bruising, or inability to void.
Pancreatic Injury Grading — AAST
Advance one grade for multiple injuries up to grade III. Proximal pancreas = to the patient's right of the superior mesenteric vein.
Grade
Type
Description
I
Hematoma
Minor contusion without duct injury
Laceration
Superficial laceration without duct injury
II
Hematoma
Major contusion without duct injury or tissue loss
Laceration
Major laceration without duct injury or tissue loss
III
Laceration
Distal transection or parenchymal injury with duct injury
IV
Laceration
Proximal transection or parenchymal injury involving ampulla
V
Laceration
Massive disruption of pancreatic head
Key CT signs: Peripancreatic fluid/stranding · Parenchymal laceration (low-attenuation line) · Ductal injury suggested by complete transection or peripancreatic fluid tracking along duct · MRCP or ERCP for definitive duct assessment. Grade III–V injuries typically require surgery or endoscopic intervention.
📋 Reporting Checklist — Pancreatic Injury
Location: head / neck / body / tail
Main pancreatic duct: intact / probable disruption / transection
AAST grade; recommend MRCP or ERCP if Grade III+ suspected
📄Radiopaedia — Pancreatic trauma
Bowel & Hollow Viscus Injury — CT Imaging
Key principle: Any free intraperitoneal air in a trauma patient without prior laparotomy = bowel perforation until proven otherwise. Bowel injury is frequently missed on initial CT — mesenteric findings often precede definitive bowel wall signs. Free fluid without solid organ injury is an important indirect sign warranting careful bowel evaluation or repeat imaging.
Finding
Significance
Notes
Pneumoperitoneum
Direct sign — perforation
Check anterior subdiaphragmatic space and perihepatic region on CT; even a tiny extraluminal bubble is significant; pneumoretroperitoneum suggests duodenal or colonic injury
Bowel wall discontinuity
Direct sign — laceration/perforation
May be subtle; inspect all bowel loops on coronal/sagittal reformats; full-thickness defect confirms perforation
Extraluminal oral contrast
Direct sign — perforation
Only if oral contrast given; highly specific; oral contrast now rarely used in trauma — absence does not exclude perforation
Mesenteric hematoma
Direct/indirect — mesenteric or bowel injury
Hyperdense blood within mesentery; may indicate vascular pedicle injury or bowel wall laceration; associated with increased risk of delayed perforation
Mesenteric stranding / fat infiltration
Indirect — mesenteric contusion or injury
Haziness and streaking in mesenteric fat; may represent contusion without perforation; serial clinical exam warranted
Bowel wall thickening
Indirect — contusion, hematoma, or ischemia
Circumferential thickening >3–5 mm; hematoma produces symmetric homogeneous thickening; ischemia produces stratified (target) pattern or loss of enhancement
Free fluid without solid organ injury
Indirect — high suspicion for bowel/mesenteric injury
Sensitivity for bowel injury ~70%; must correlate with clinical exam and mechanism; isolated free fluid in blunt trauma = diagnostic laparoscopy consideration
Bowel wall hyperenhancement or non-enhancement
Direct — active hemorrhage or devascularization
Focally absent enhancement = ischemia/infarction; active extravasation = arterial blush within bowel wall
Segment-specific pearls: Duodenum — retroperitoneal position; look for pneumoretroperitoneum, peripancreatic hematoma, duodenal wall thickening; seat-belt mechanism; associated pancreatic injury common. Small bowel — most commonly injured hollow viscus in blunt trauma; lap belt injury pattern (Chance fracture + bowel injury). Colon — less commonly injured bluntly; consider penetrating mechanism; ascending and sigmoid most vulnerable.
Key principle: Do not withhold indicated imaging — maternal health is critical to fetal health. Typical trauma CT (abdomen/pelvis) delivers ~25 mGy to the fetus, well below the 50 mGy safety threshold. Prompt diagnosis of maternal injury protects both mother and fetus. IV iodinated contrast is safe in pregnancy (FDA Category B). Gadolinium: avoid unless benefits clearly outweigh fetal risk (FDA Category C).
Clinical algorithm: Hemodynamically unstable + FAST positive → laparotomy without further imaging delay. Hemodynamically stable: FAST first → if positive for free fluid or signs of peritonitis → CECT abdomen/pelvis. If FAST negative but clinical concern remains → CECT if indicated. US useful for targeted fetal assessment and gestational age confirmation at any stage. Laparotomy vs. observation in stable patients may be guided by CT findings and gestational age (>24 weeks → fetal monitoring).
Obstetric Injuries — Placental Abruption
Most important obstetric injury: Occurs in 20–50% of pregnant patients experiencing major trauma. Second most common cause of fetal death after maternal shock. US sensitivity is low — 50–80% of traumatic abruptions are missed prospectively at initial US. External fetal monitoring is more sensitive than US for abruption detection and should always be performed for at least several hours after trauma (even seemingly minor trauma, as 1–5% of "minor" cases result in abruption).
Feature
CT Findings
US Findings
Acute hematoma / abruption
Heterogeneous placenta; area(s) of hypoattenuation or nonenhancement; retroplacental hyperattenuating blood; large retroplacental hematomas undermine placental tissue
Retroplacental collection (hyperechoic acutely, becomes hypoechoic / isoechoic as hemorrhage evolves — improving conspicuity on follow-up US)
Cotyledons, venous lakes, chorionic plate indentations, age-related infarcts — may mimic hypoattenuation. Geographic hypoattenuation is NOT specific for abruption.
Prominent venous lakes may mimic retroplacental hematoma — correlate with CT
Complete abruption
Total absence of placental perfusion/enhancement; associated hemoperitoneum
Avascular placenta on Doppler; absent or abnormal fetal cardiac activity
Rupture of membranes
Large volume of fluid in vagina with low volume of residual amniotic fluid; heterogeneous placenta
Grades based on degree of placental enhancement on CECT. Intended for 2nd and 3rd trimester. Clinical diagnosis of abruption must be present for grading to apply.
Grade
Placental Enhancement
Clinical Management
0
100% — homogeneous normal enhancement
Normal; expectant management; good clinical outcomes expected
1
>50% — small geographic hypoattenuation (likely normal variants: cotyledons, venous lakes, age-related infarcts)
Normal; expectant management; good clinical outcomes expected
2a
>50% — nongeographic hypoattenuation, full thickness, acute angles with myometrium
Increased probability of abruption; extended clinical monitoring recommended
2b
25–50% — larger area of decreased enhancement
Increased probability of abruption; extended clinical monitoring recommended
3
<25% — near-complete devascularization
Fetal death occurs frequently; consider immediate cesarean delivery if abruption confirmed
Uterine Rupture
Feature
Details
Incidence & significance
~0.6% of trauma in pregnancy; fetal mortality approaches 100%; maternal mortality ~10% (not typically the primary injury causing maternal death)
CT findings
Myometrial wall defect (most commonly fundus or anterior uterine wall); fetal parts external to uterine contour; hemoperitoneum; complex fluid adjacent to perforation site; diffusely heterogeneous uterus
US findings
Uterine contour defect; fetal parts outside uterus; intraperitoneal fluid; may be used intraoperatively
Risk factors
Prior cesarean delivery; prior uterine surgery; congenital anomalies; scarring. Blunt and penetrating mechanisms both implicated.
Fetal Injuries
Injury
Details
Direct fetal injury
Rare (<1% of trauma cases). Fetus relatively protected in 1st trimester by pelvic bones. Risk increases with gestational age as fetus grows and head may engage the pelvis.
Fetal skull fractures
CT more sensitive than US for bone detail. Fetal death in up to 35% when pelvic fracture present. Linear nondisplaced — monitoring without surgical intervention. Depressed fractures — percutaneous or surgical elevation. Fetal ICH may be associated.
Fetal intracranial hemorrhage
Identifiable on CT; associated with skull fractures; deceleration mechanism. Intrauterine fetal death may result.
Rib / long bone fractures
May be seen on CT with severe pelvic trauma or direct compression. Multiple fetal fractures raise concern for severity of impact.
Penetrating trauma
Gravid uterus provides protection by displacing abdominal organs; uterine musculature slows projectiles. Severe fetal injury in 60–70% of penetrating trauma; fetal mortality 71–73% with gunshot wounds to the gravid uterus.
Displaced superiorly by gravid uterus; splenomegaly from increased blood volume → increased susceptibility to rupture from blunt or penetrating trauma
Liver
Displaced superiorly and compressed against rib cage; higher risk of laceration
Bowel
Displaced peripherally by uterus; increased risk of injury with penetrating trauma (less protection by uterus laterally)
Bladder
Elevated out of pelvis by gravid uterus; extraperitoneal rupture common (peritoneal reflection is below the displaced bladder). CT cystography or delayed CT imaging recommended if pelvic fracture + hematuria or clinical suspicion.
Pelvic fractures
Maternal mortality up to 9%. Pelvic fracture is not an absolute contraindication to vaginal delivery but increases risk of fetal skull fracture if head is engaged. Fetal death in up to 35% when pelvic fracture present.
Vascular
Increased pelvic blood flow → higher risk of severe hemorrhage after blunt or penetrating pelvic trauma
📋 Reporting Checklist — Trauma in Pregnancy
Placenta: estimate percentage of normal enhancement (TAPS grade if 2nd/3rd trimester); retroplacental or marginal hematoma; size of hypoattenuating area
Myometrium: wall contour intact or defect present; fetal parts within or outside uterine contour
Amniotic fluid: volume (oligohydramnios / anhydramnios); fluid in vagina (premature rupture of membranes)
Fetal: position (cephalic / breech / transverse); estimated gestational age; skull fractures; intracranial hemorrhage; long bone or rib fractures
Free fluid: intraperitoneal location and density (HU consistent with blood); hemoperitoneum volume estimate
Pelvic ring: fracture type; acetabular involvement; proximity to fetal head
Bladder: wall integrity; extravasation on delayed images; cystography findings if performed
📄Langdon JH, Chai N, Patel A, et al. Imaging of Trauma in Pregnant Patients. RadioGraphics. 2025;45(10):e240043. https://doi.org/10.1148/rg.240043
Gunshot Injuries
Ballistic fundamentals: Low-velocity (<2,000 fps) — handguns and most civilian firearms. Injury from permanent cavitation (tissue crushed directly by projectile) only. Tissue destruction limited to projectile diameter + fragmentation. High-velocity (>2,000 fps) — rifles and military weapons. Add temporary cavitation: pressure wave expands a transient cavity far larger than the bullet diameter, causing indirect injury to structures not directly contacted. Organs tolerating stretch (lung, muscle) handle this better than those that do not (brain, liver, spleen, kidney, bowel). Shotgun — range-dependent: close range (<3 m) delivers high-energy injury comparable to rifle; intermediate range produces spreading pellet pattern; distant range (>7 m) deposits pellets in subcutaneous tissue only.
Secondary projectiles: Bullet fragments and bone chips driven off by impact become high-velocity secondary missiles, extending the zone of injury well beyond the primary bullet path. When a bullet strikes cortical bone, resulting bone fragments can lacerate adjacent neurovascular structures, even if the primary projectile did not directly contact them. Always evaluate structures adjacent to any bone impact site.
CT Trajectory Assessment — Structures to Evaluate by Zone
Vertebral body fracture/comminution; intracanalicular bullet or bone fragment; epidural hematoma; bullet trajectory crossing midline predicts cord injury; paraspinal hematoma
Extremities (MSK)
Long bones, major arteries/veins, peripheral nerves, joints, compartments
Comminuted fracture with bone fragment dispersal; periosteal stripping; intraarticular fragments; expanding soft tissue hematoma; absent distal flow on CTA; compartment syndrome (muscle edema, obliteration of fat planes)
Intraarticular Bullet / Fragment
Report explicitly — clinical consequences are high: Lead toxicity: Synovial fluid is mildly acidic and dissolves lead → systemic absorption → plumbism (anemia, encephalopathy, neuropathy). Risk is highest when the bullet is within a synovial joint or bursa; fragments in soft tissue or bone carry lower but real risk if near vascular structures. Joint sepsis: Bullet carries skin flora along the tract; intraarticular entry creates a direct pathway for infection. Articular cartilage injury: Metallic debris and bone chips cause mechanical damage and degenerative change.
Surgical extraction is generally indicated for intraarticular projectiles.
Retained Projectile — MRI Considerations
Most civilian lead bullets and copper-jacketed rounds are non-ferromagnetic and are generally considered MRI-conditional or safe. Steel-jacketed military rounds (full metal jacket with steel core) may be ferromagnetic — obtain prior radiographs to assess composition before MRI.
Metallic fragments in or near the orbit, spinal canal, or major vessels are high-risk regardless of composition. MRI artifact (susceptibility) can limit evaluation of adjacent structures — CT may be preferred for trajectory assessment near retained fragments.
📋 Reporting Checklist — Gunshot Injuries
Projectile accounting: number visible on scout/XR; correlate with entry/exit wounds to determine retained vs. passed through
Trajectory: describe projected path (entry zone → exit zone or retained location); note crossing midline, traversing body cavities, proximity to named structures
Bone injury: fracture pattern, degree of comminution; bone fragment dispersal (secondary missiles); periosteal stripping
Intraarticular involvement: bullet or fragment within joint space — specify joint; note articular surface injury
Vascular: expanding hematoma, pseudoaneurysm, occlusion, active extravasation (CTA if trajectory near major vessels)
Hollow viscus: free air, mesenteric stranding/hematoma, bowel wall discontinuity (GI perforation → high infection risk from bacterial seeding along tract)
Compartment syndrome: muscle edema, loss of fat plane definition, fascial integrity; flag if trajectory through a tight compartment (leg, forearm, thigh)
Retained foreign material: location (intraarticular / soft tissue / bone / vascular / spinal canal); MRI safety note if relevant
Recommended additional imaging: CTA for vascular injury, CT cystogram for pelvic trajectory near bladder, MRI spine for cord compression
📄Sodagari F et al. Gunshot Wounds: Mechanisms, Radiologic Manifestations, and Complications. RadioGraphics. 2020;40(6):1756–1788.
Other
Acute Appendicitis
CT criteria: Appendix diameter >6mm (outer wall to outer wall) + wall thickening + periappendiceal fat stranding. Appendicolith present in ~30% (increases perforation risk). MRI preferred in pregnancy and pediatrics. CT sensitivity ~94%, specificity ~95%.
Finding
CT
US
Notes
Appendix diameter >6mm
Outer wall–outer wall; distended with fluid
Non-compressible tubular structure >6mm
Primary criterion; measure at widest point
Periappendiceal fat stranding
Haziness/streaking in periappendiceal fat
Echogenic surrounding fat
Increases specificity when combined with dilation
Appendicolith
Calcified focus within appendiceal lumen; extraluminal if perforated
Shadowing echogenic intraluminal focus
~30% of cases; associated with perforation/gangrene
Wall enhancement/thickening
Stratified wall enhancement; wall >2mm
Hyperechoic mucosa with thickened layers
Loss of enhancement = gangrenous/necrotic wall
Perforation signs
Free air (RLQ), periappendiceal abscess (rim-enhancing collection), phlegmon
Free fluid RLQ; disrupted wall layers
Perforation rate ~20–30%; IR drainage for abscess >3cm
Non-visualization
May be normal (retrocecal, pelvic) or suggest alternative diagnosis
Non-visualization common (~20–30%); proceed to CT in adults
Always report explicitly — do not call normal
Perforated appendicitis: Localized free extraluminal air in RLQ · Periappendiceal abscess · Phlegmon (ill-defined mass without discrete rim) · Free fluid in RLQ/pelvis. Gangrenous appendicitis: Absent mural enhancement · Intraluminal gas · Focal wall defect. Both require urgent surgical or IR consultation.
Pearls: State diameter + fat stranding + appendicolith separately in report. Retrocecal appendix (~26%): may present with flank pain — ensure full coronal/sagittal review. Tip appendicitis: isolated inflammation of the tip, may be subtle.
Critical finding: Pneumatosis intestinalis (intramural gas) + portal venous gas = grave prognosis — indicates advanced bowel necrosis with transmural infarction. Report immediately and obtain urgent surgical consultation. Distinguish pneumatosis from intraluminal gas: pneumatosis follows bowel wall contour, seen on multiple planes, often linear or bubbly in pattern.
SMA embolus vs thrombosis: SMA embolus: filling defect typically 3–10 cm from SMA origin (beyond origin at middle colic artery), often cardiac source (Afib, endocarditis); spares proximal jejunum. SMA thrombosis: occlusion at or near SMA origin, atherosclerotic disease, ischemia of entire SMA territory including proximal jejunum; longer segment ischemia; prior intestinal angina history.
Etiology
CT Findings
Territory
SMA occlusion — embolus
Filling defect in SMA 3–10 cm from origin; bowel wall thickening → thinning (necrosis); pneumatosis; portal venous gas; lack of bowel wall enhancement; mesenteric stranding
Mid-jejunum to transverse colon; spares proximal jejunum and duodenum (SMA branches beyond origin occluded)
SMA occlusion — thrombosis
Atherosclerotic calcification/plaque at SMA origin; near-complete or complete occlusion at origin; extensive small bowel and right colon ischemia; collateral vessels may be visible
Entire SMA territory including proximal jejunum; duodenum may be involved; longer ischemic segment than embolus
SMV thrombosis
Hyperdense SMV (acute thrombus); filling defect in SMV ± portal vein; mesenteric edema and ascites (venous congestion); bowel wall thickening (target sign/halo); hemorrhagic infarction more common than arterial; pneumatosis less common early
Variable; often patchy; mesenteric venous distribution; may spare arterially supplied areas; hypercoagulable states, portal hypertension, pancreatitis
Non-occlusive mesenteric ischemia (NOMI)
Patent mesenteric vessels; diffuse bowel wall thickening; poor bowel wall enhancement; mesenteric edema; no filling defect; SMA vasospasm may be visible on angiography
Watershed areas most vulnerable: splenic flexure, sigmoid; diffuse distribution possible; ICU/low-flow states, dialysis, vasopressors
Colonic ischemia (watershed)
Bowel wall thickening ± thumbprinting (submucosal edema); pericolonic stranding; watershed zones; typically no occlusion on CT; pneumatosis in severe cases
Splenic flexure (Griffiths point) and rectosigmoid junction (Sudeck point) — watershed zones between SMA/IMA and IMA/internal iliac territories
Strangulation / closed-loop
Closed loop morphology + wall thickening + loss of enhancement + mesenteric engorgement + ascites + pneumatosis; combination of arterial and venous compromise due to twisting
Isolated closed loop; variable size; sigmoid or internal hernia most common; rapidly progressive to full-thickness necrosis
📄Menke J. Diagnostic accuracy of MDCT for acute mesenteric ischemia: A systematic review. Eur Radiol. 2010;20(12):2805-14.
Closed loop obstruction — surgical emergency: Two adjacent transition points creating an isolated loop with no decompression. Signs: C- or U-shaped dilated loop, mesenteric swirl (twisted mesentery), beak sign (tapered ends at transition), whirl sign (twisting of mesenteric vessels/fat), dilated loop with wall thickening or pneumatosis. Requires urgent surgical consultation regardless of other findings.
Caliber thresholds: SBO: dilated loops >2.5 cm proximal to transition point with decompressed loops distally. LBO: colon >6 cm (cecum >9 cm = impending perforation / Ogilvie risk). Water-soluble contrast enema or CT colonography can characterize LBO level and etiology. Pneumoperitoneum = perforation.
Feature
SBO (Small Bowel)
LBO (Large Bowel)
Location
Central abdomen; jejunum (left upper) vs ileum (right lower)
Peripheral/frame-like distribution of dilated colon
Caliber threshold
>2.5 cm (small bowel); >3 cm (duodenum)
>6 cm colon; >9 cm cecum = imminent perforation risk
Emphysematous cholecystitis: Gas in the gallbladder wall (intramural) or lumen on CT = gas-forming organisms (Clostridium, E. coli). Seen in diabetics, elderly, vascular disease. High mortality (15–25%) — emergent cholecystectomy (percutaneous cholecystostomy if too ill). Do not confuse with intraluminal gas (normal post-procedure) — intramural gas follows wall contour, non-dependent, linear/bubbly.
Distended bowel loops; large ectopic gallstone; biliary-enteric fistula (pneumobilia); may show cholecystoduodenal fistula
Rigler's triad: SBO + ectopic gallstone + pneumobilia; stone typically at terminal ileum (narrowest point); Bouveret syndrome = gastric outlet obstruction (duodenal impaction)
Urgent surgical enterolithotomy; fistula repair at same or staged procedure depending on patient stability
Mirizzi syndrome
Impacted stone in GB neck/cystic duct causing extrinsic compression of CHD; proximal biliary dilatation with normal distal CBD; gallbladder contracted
Stone impacted at GB neck; fusiform narrowing of CHD/CBD at cystic duct level; biliary dilatation above; choledochal fistula in advanced cases (type II–IV)
Urgent — high surgical complexity; ERCP pre-op for biliary drainage; cholecystectomy ± biliary reconstruction; distinguish from malignancy (Klatskin tumor)
📄Shakespear JS et al. CT findings of acute cholecystitis and its complications. AJR. 2010;194(6):1523-9.
Rim-enhancing fluid collection adjacent to or distant from colon; may contain gas
>3–4 cm = IR percutaneous drainage; elective sigmoid resection 6–8 weeks later
Fistula
Colovesical: air/fecal matter in bladder · Colovaginal: air in vagina
Surgical repair after bowel prep; colovesical most common
Obstruction
LBO/SBO from extrinsic compression by phlegmon or fibrosis
NG decompression; surgical consult if complete
Surgical emergency: Free air + diffuse peritoneal enhancement = Hinchey IV. Always report free intraperitoneal air with diverticulitis — even small amounts change management.
Ruptured ectopic — hemorrhagic emergency: Free pelvic/abdominal fluid + positive β-hCG = ruptured ectopic until proven otherwise. Do NOT delay for MRI. Hemodynamically unstable patient goes directly to OR. Hemodynamically stable: US to confirm. Hemoperitoneum extending to Morrison's pouch or paracolic gutters = large hemorrhage.
Heterotopic pregnancy: Simultaneous intrauterine and ectopic pregnancy. Rare in general population (~1:30,000) but significantly increased with ART (~1:100–500). Presence of an intrauterine pregnancy does NOT exclude a co-existing ectopic. Always evaluate adnexa even when IUP is confirmed in ART patients.
Finding
Description
Empty uterus with β-hCG >1500–2000 mIU/mL
Discriminatory zone: β-hCG above which IUP should be visible on TVUS (1500–2000 mIU/mL for TVUS; 6500 mIU/mL for transabdominal). Empty uterus above discriminatory zone = ectopic or failed IUP. Note: heterotopic can have IUP + ectopic simultaneously.
Trophoblastic "ring of fire" Doppler signal around ectopic sac; echogenic ring on B-mode ("bagel sign"); distinct from the ovary (surrounded by ovarian parenchyma = corpus luteum cyst); TVUS most sensitive
Round or oval adnexal structure separate from ovary; may contain yolk sac or embryo (definitive diagnosis); Doppler: "ring of fire" around ectopic sac (trophoblastic flow)
Free pelvic fluid (hemorrhage)
Non-dependent echogenic free fluid in cul-de-sac, Morrison's pouch, paracolic gutters; complex/echogenic = hemoperitoneum; simple free fluid less specific; volume correlates with degree of hemorrhage
Interstitial ectopic
Gestational sac within myometrium at cornual region; interstitial line sign (echogenic line connecting ectopic sac to endometrium); thin myometrial rim <5 mm; presents later (8–12 weeks) with greater hemorrhage risk than tubal ectopic; 2–4% of ectopics; high mortality
📄Barnhart KT. Ectopic pregnancy. N Engl J Med. 2009;361(4):379-87.
Myometrial rim thickness if interstitial (<5mm = high rupture risk)
Heterotopic pregnancy consideration if ART patient
Epiploic Appendagitis & Omental Infarct
Clinical importance: Both are self-limiting conditions treated conservatively (NSAIDs, analgesia). Both clinically mimic appendicitis or diverticulitis. CT is diagnostic and avoids unnecessary surgery and antibiotics. Report confidently when findings are characteristic to prevent unnecessary admission or intervention.
Feature
Epiploic Appendagitis
Omental Infarct
Location
Immediately adjacent to colon wall (sigmoid most common, then cecum/ascending); antimesenteric border
Larger area of right-sided omentum most common (right lower quadrant > right upper quadrant); not directly attached to colon
Size
Small, ovoid; typically 1.5–3.5 cm; proportional to appendage size
Larger; typically >3–5 cm; cake-like fatty mass; may be very large (>10 cm)
Central hyperdense dot
Central hyperdense focus (thrombosed central vessel) within fatty lesion — characteristic sign (~70%)
Absent (no central vessel); heterogeneous fatty stranding without central dot
Fat stranding pattern
Oval pericolonic fat with thin hyperattenuating rim (inflamed/thrombosed epiploic appendage); surrounding inflammation limited
Diffuse, cake-like omental fat stranding; less well-defined; no discrete rim; larger area of involvement
Self-limiting
Yes — resolves in 2–4 weeks; rarely recurs; conservative management
Yes — resolves in 4–6 weeks; conservative management; rarely requires surgery for refractory cases
📄Singh AK et al. Omental infarct and epiploic appendagitis: imaging characteristics and treatment. Emerg Radiol. 2005;11(2):82-7.
Ultrasound findings: Enlarged ovary (>4 cm, often >5 cm); peripheral follicles displaced to periphery (hallmark — "string of pearls"); ovary displaced from normal position (may be midline or contralateral); absent or decreased Doppler flow; free pelvic fluid; associated adnexal mass (dermoid, cystadenoma) in ~50–60% of cases; thickened edematous stroma.
Critical pitfall: Normal Doppler flow does NOT exclude ovarian torsion. Intermittent torsion or partial torsion can preserve some flow. Clinical presentation + enlarged ovary + peripheral follicles = high suspicion regardless of Doppler. This is a surgical emergency — diagnostic laparoscopy if clinical suspicion is high. Delay causes ovarian infarction and loss.
Pearls: Right > left (sigmoid colon limits left ovarian mobility). Associated ovarian mass in ~50–60% of cases — teratoma, cystadenoma most common. Pediatric patients: torsion can occur with normal ovaries. MRI if equivocal US — T2 hyperintense edematous stroma, absent enhancement in late/infarcted torsion. Doppler twisting of vascular pedicle ("whirlpool sign") is specific but not always present.
📄Shadinger LL et al. Preoperative sonographic and clinical characteristics as predictors of ovarian torsion. J Ultrasound Med. 2008;27(1):7-13.
Contralateral ovary: normal / abnormal (volume and flow)
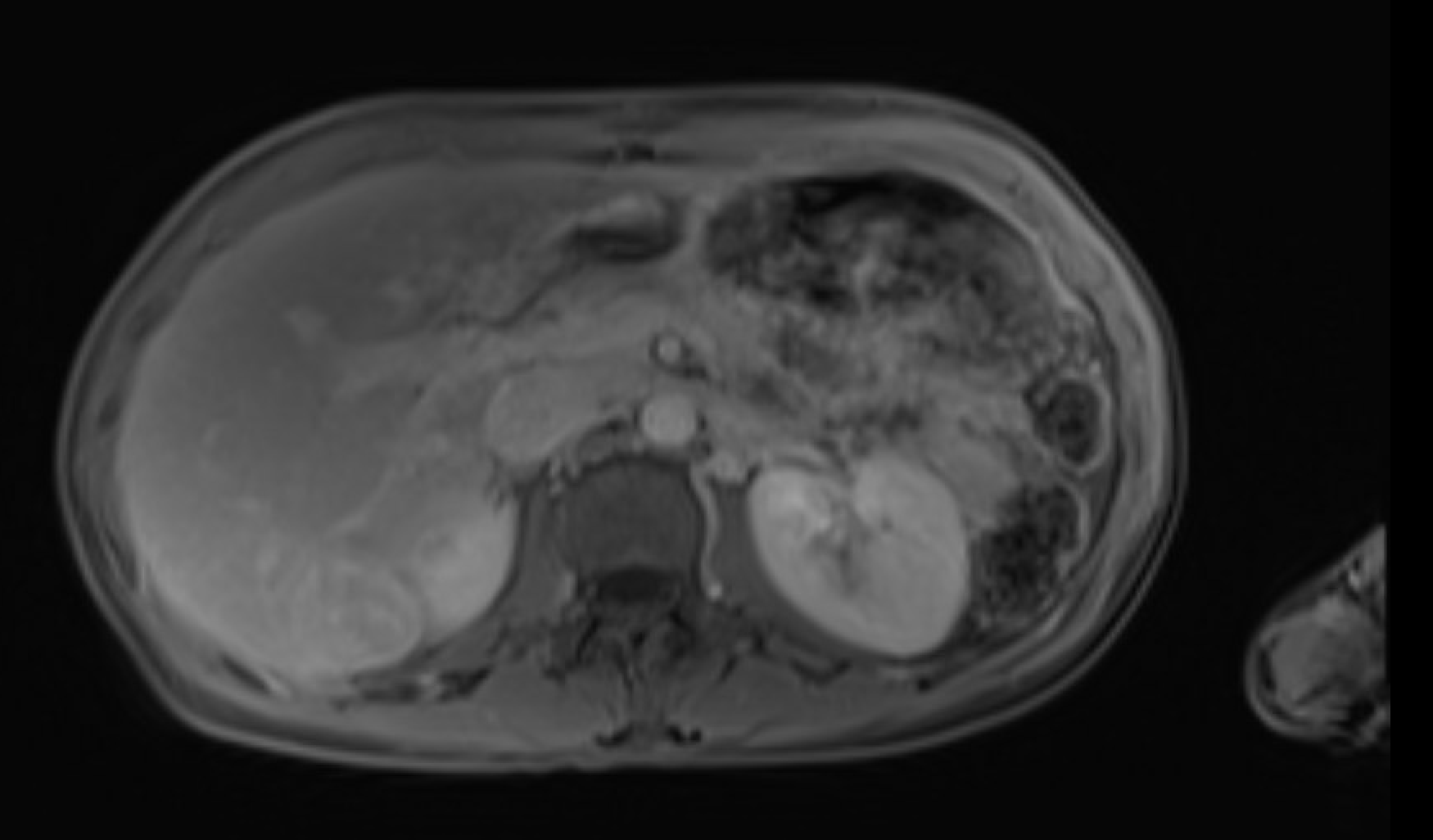
Pancreatitis
Revised Atlanta Classification: Interstitial edematous pancreatitis vs. necrotizing pancreatitis (parenchymal and/or peripancreatic necrosis). CT should be performed ≥48-72h after onset for accurate necrosis assessment.
Sigmoid volvulus: Massively dilated sigmoid colon >6 cm, apex pointing toward RUQ ("coffee bean" or "bent inner tube" pointing right), loss of haustral markings, convergence of walls at twist site. Cecal volvulus: ileocecal junction identified out of position (cecum absent from RLQ), dilated cecum in left upper abdomen, "coffee bean" opening toward LUQ. Both require urgent decompression or surgery.
Type
Imaging Signs
Notes
Sigmoid volvulus
Massively dilated inverted U-shaped sigmoid loop; apex points to RUQ; "coffee bean" or "bent inner tube" sign on XR; convergence of walls at left pelvis (twist site); loss of haustra; CT: whirl sign at twist, beak sign, dilated sigmoid >6 cm; often massive colonic dilation
Most common volvulus (60–75%); elderly/institutionalized patients; chronic constipation; sigmoid redundancy; endoscopic decompression often successful; high recurrence; sigmoidectomy definitive
Cecal volvulus
Cecum absent from RLQ; dilated ovoid gas-filled cecum in left mid-abdomen or LUQ; "coffee bean" opening toward LUQ; small bowel dilation; CT: whirl sign at ileocecal junction; cecum >10 cm; dilated terminal ileum; appendix may be visible with cecum
Second most common volvulus (25–40%); younger patients; congenital lack of retroperitoneal fixation; right hemicolectomy required; endoscopic decompression generally not definitive; high failure/recurrence rate; cecal bascule variant (folding without twisting)
Gastric volvulus — organoaxial
Stomach rotates around long axis (cardiopyloric axis); greater curvature flips superiorly; two air-fluid levels on upright CXR (double bubble); inversion of stomach; NGT cannot be passed; associated with diaphragmatic defect
More common type; associated with paraesophageal/diaphragmatic hernia; Borchardt triad: severe epigastric pain + retching without vomiting + inability to pass NGT; surgical emergency if strangulation
Gastric volvulus — mesenteroaxial
Rotation around short axis (perpendicular to cardiopyloric axis); antrum rotates anteriorly and superiorly; intermittent symptoms; partial obstruction pattern
Less common; often intermittent and partial; associated with diaphragmatic eventration; may reduce spontaneously; surgical repair of predisposing defect
📄Peterson CM et al. Volvulus of the gastrointestinal tract. AJR. 2009;192(2):W105-15.
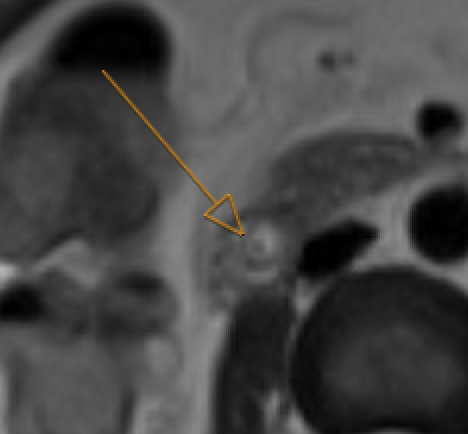
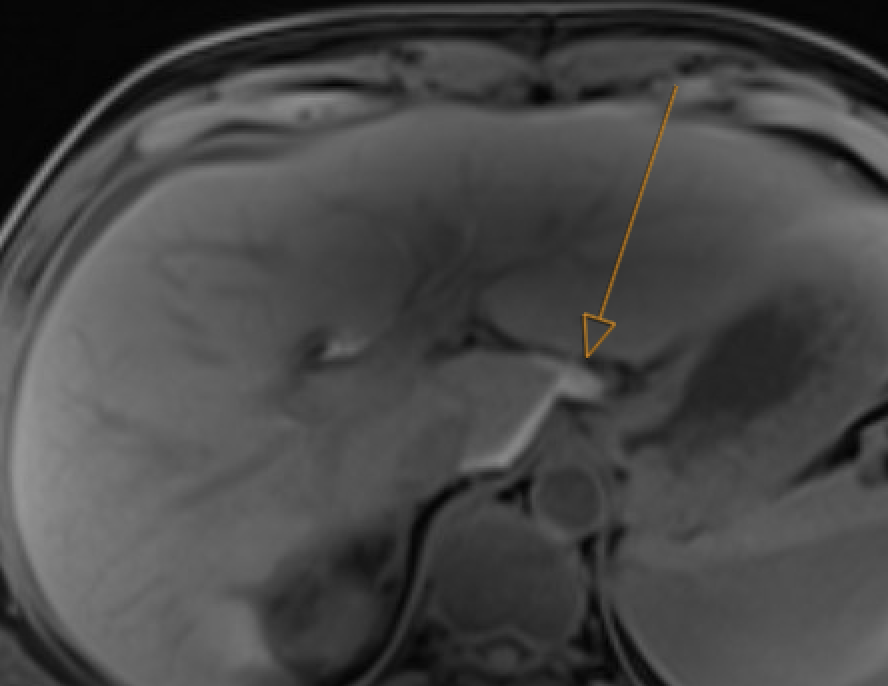
T2-hypointense filling defect in bile duct on MRCP. Obstructive: upstream dilatation, abrupt caliber change. Trace entire biliary system on thin MRCP/T2W
Choledocholithiasis: T2-dark filling defect (arrow) on MRCP
GB neck and cystic duct are blind spots. Pneumobilia can mimic calculi (nondependent, blooms on GRE). Crossing vessel on coronal MRCP can mimic filling defect — check axial reformats
Abscess: rim enhancement + central DWI restriction. Hematoma: central DWI restriction but no rim enhancement + T1 hyperintensity
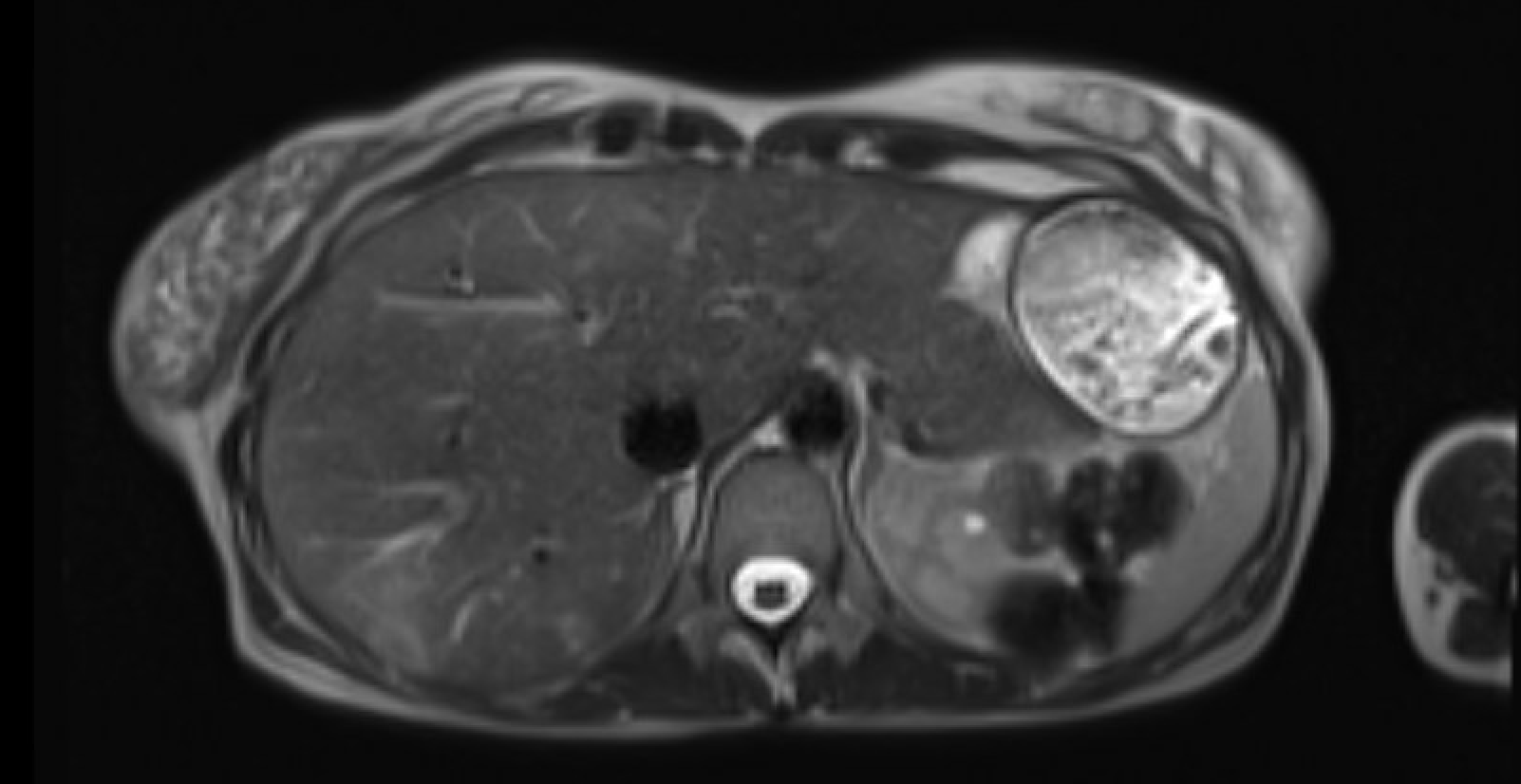
Hemorrhagic cholecystitis
Distended GB with T1-hyperintense and T2-hypointense contents; blooming on T2* GRE; active bleed on subtraction images. No enhancement within hematoma itself
T1W: hyperintense blood products
Both hemorrhage and inspissated bile are T1-bright — use GRE blooming to distinguish. Check subtraction images for active extravasation
T2W MRCP: delineate anatomy. Gadoxetate (Eovist) hepatobiliary phase: extravasation of excreted contrast from duct into collection. Add 60–90 min delayed phase if 20–30 min scan is negative
20 min HBP: leak site identifiedDelayed: extravasation confirmed
Avoid gadoxetate if bilirubin >3 mg/dL, severe hepatic failure, or competing drugs (methotrexate, tamoxifen, cisplatin)
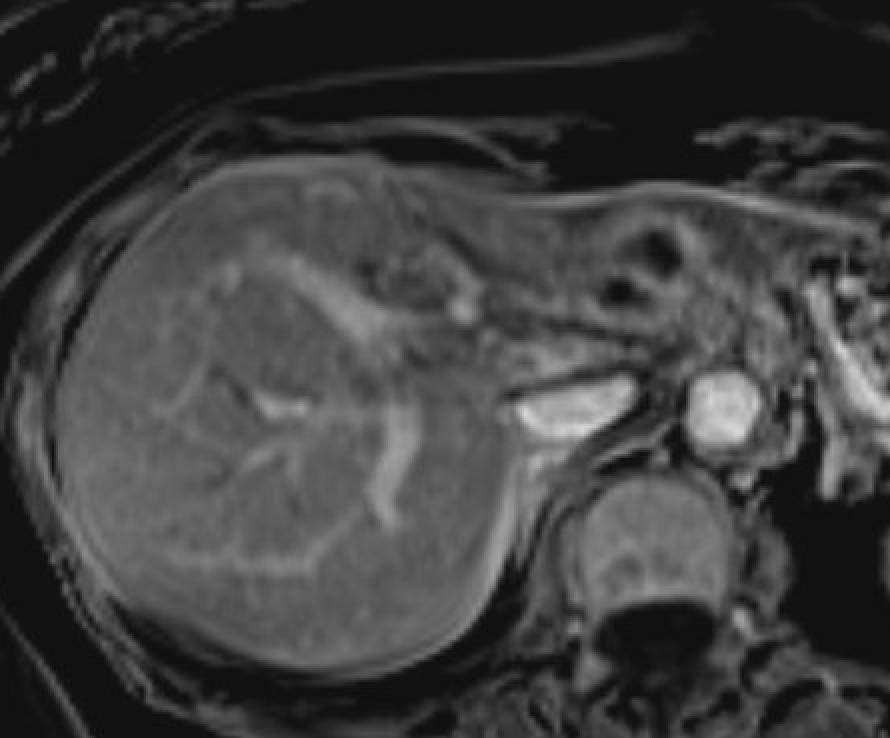
Rim-enhancing collection + central diffusion restriction; double-target sign; perilesional hyperemia (arterial phase)
Hepatic abscess: rim enhancement
Overlaps with cystic metastases — abscess favored by clinical context (fever, leukocytosis, recent biliary intervention). Short-term follow-up if unclear
Hemorrhagic hepatic lesion
Lesion with T1-hyperintense and T2-hypointense blood products; blooming on GRE; nonenhancing hemorrhagic component on subtraction. Look for enhancing viable tumor around hematoma
HCC: check for tumor-in-vein (thrombus enhances like primary tumor). Adenoma: young women, OCP use, peripheral enhancement pattern. Subtraction mandatory when T1 hyperintensity is present
Quick Reference: Peliosis Hepatis vs. Hepatic Abscess
⚠ Critical safety note: Misdiagnosing peliosis hepatis (PH) as abscess and performing percutaneous drainage can cause life-threatening hemorrhage from the blood-filled sinusoidal cavities. When imaging is equivocal, biopsy (transjugular preferred) rather than drainage.
Feature
Peliosis Hepatis
Hepatic Abscess
Clinical
Usually incidental/asymptomatic (70–92%); associated condition (malignancy, steroids, OCP, HIV). Normal or mildly elevated LFTs. No fever.
Bacillary peliosis (Bartonella henselae in HIV/AIDS) can present with fever mimicking abscess — but shows the vascular fill-in pattern. Responds to erythromycin or doxycycline.
Management:
Abscess suspected: Image-guided aspiration for culture ± drainage
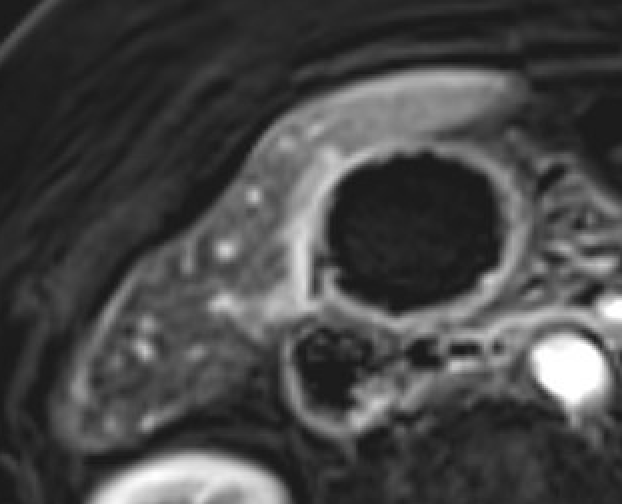
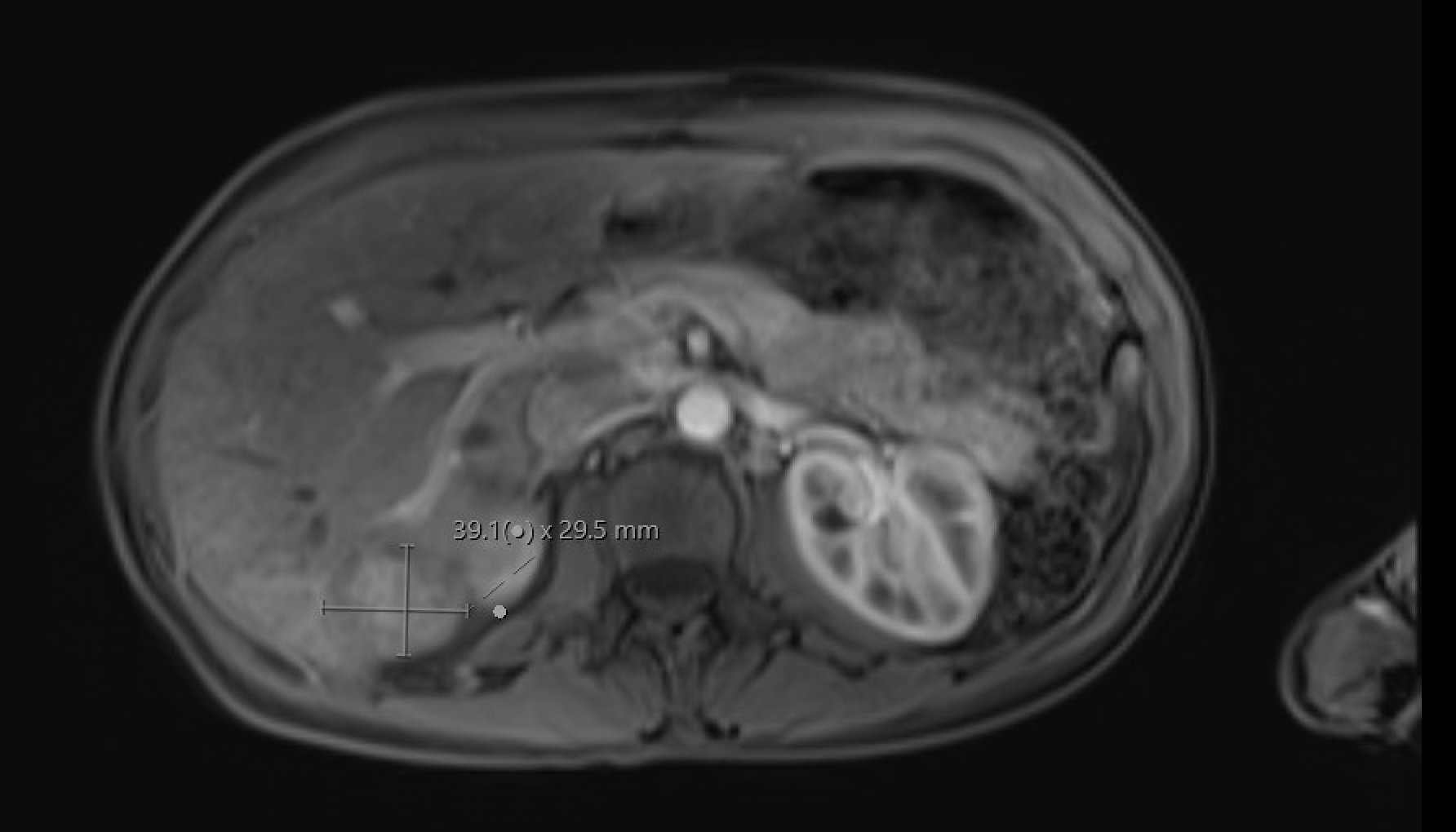
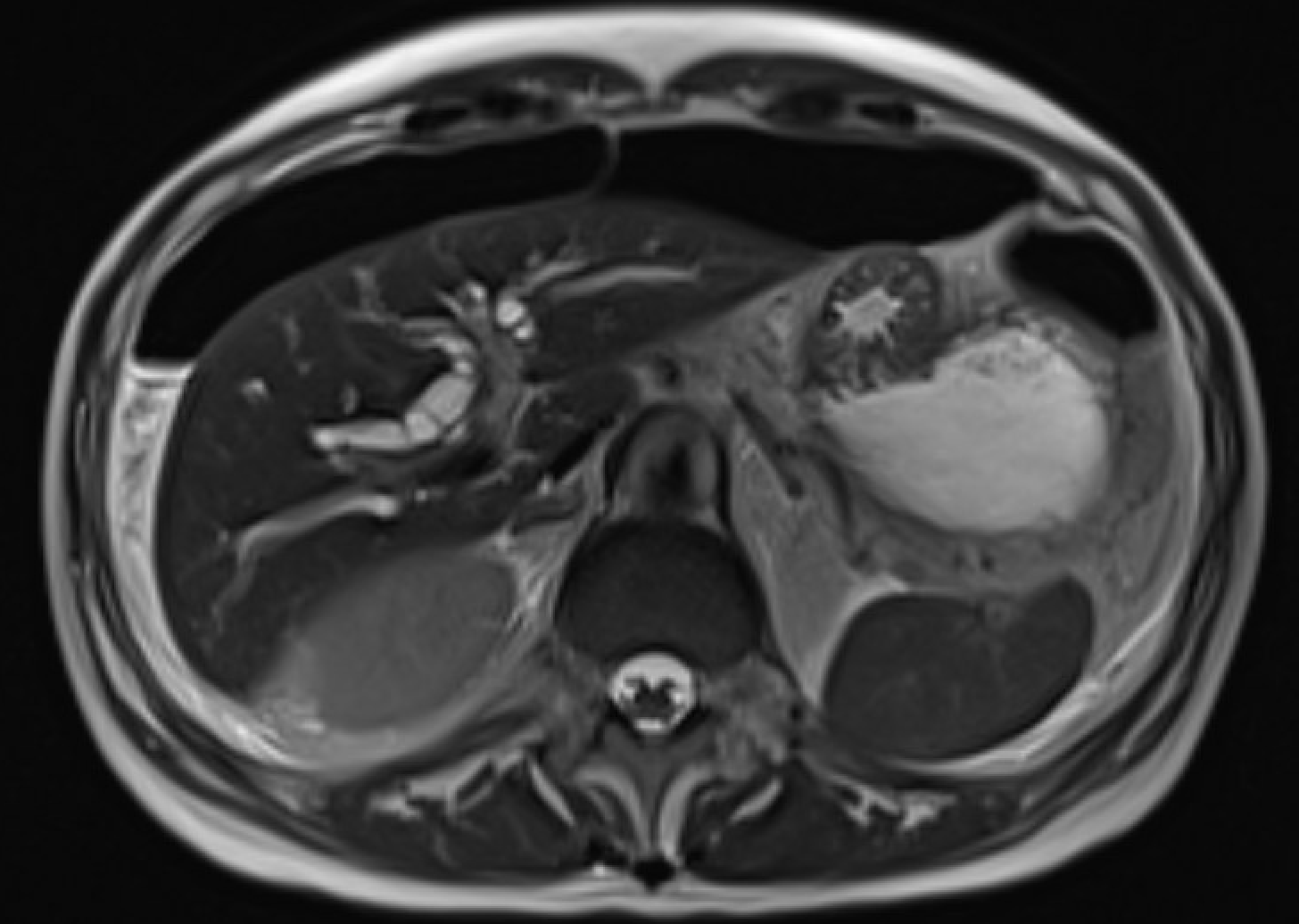
Pancreatic edema (loss of normal T1 hyperintensity) + peripancreatic fluid on T2W + preserved parenchymal enhancement on post-Gd
IEP: loss of T1 signal, preserved enhancement, peripancreatic fluid
Normal pancreas is T1-bright (brighter than liver). Loss of T1 signal = edema/inflammation. DWI restriction is sensitive for early pancreatitis. India ink artifact on out-of-phase shows subtle fat stranding
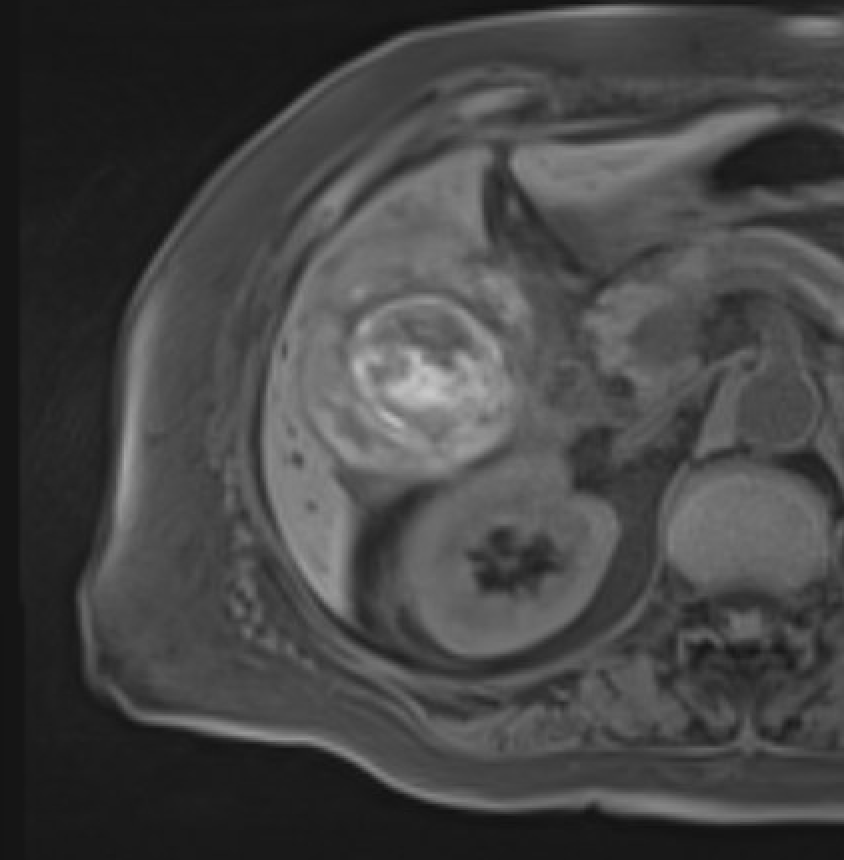
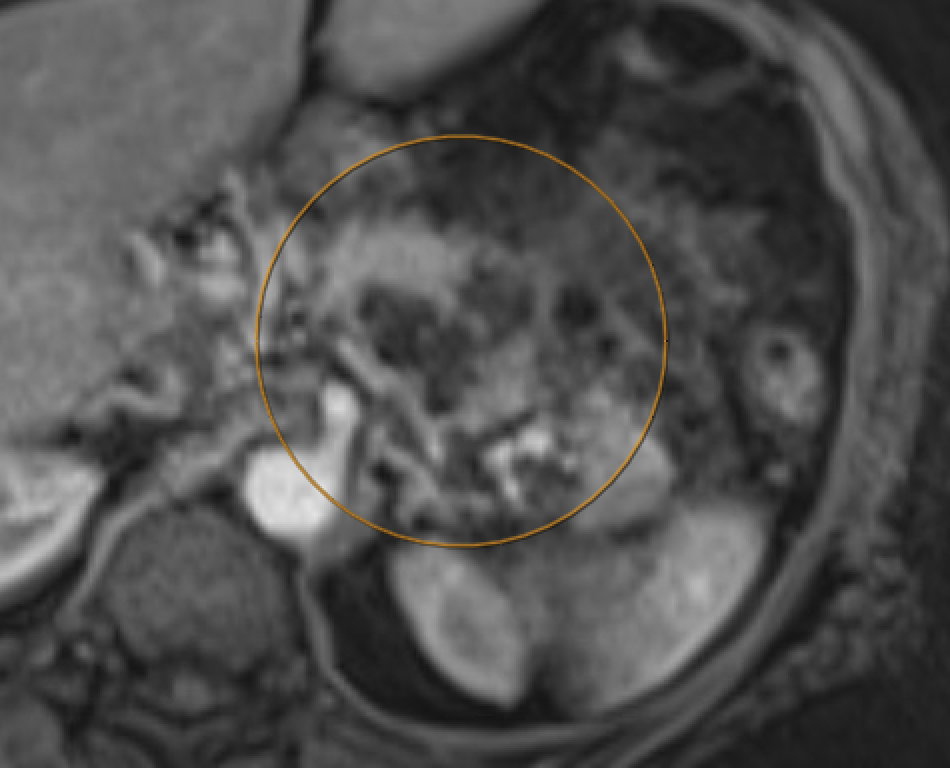
Lack of parenchymal enhancement on post-Gd = necrosis. Hemorrhage: T1 hyperintensity + GRE blooming. Vascular complications: thrombosis (filling defect on bSSFP/post-Gd), pseudoaneurysm
Necrotizing pancreatitis: nonenhancing parenchyma = necrosis
Pitfall: Diffuse hemorrhagic necrosis can appear T1-bright, mimicking normal pancreas. Always check post-Gd for absent enhancement and T2W for necrosis
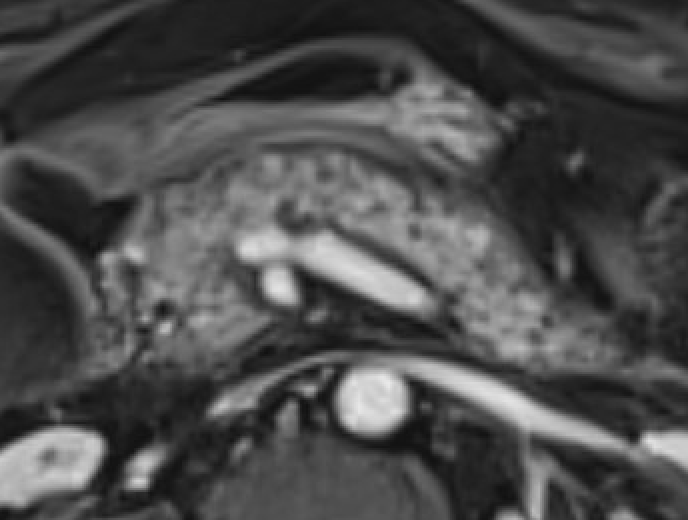
Pancreatic trauma
Full-thickness laceration = T2-hyperintense linear signal disrupting parenchyma. Trace pancreatic duct on T2W axial images (MRCP often limited by surrounding fluid)
Ductal injury (AAST Grade III+) = surgical indication. MRI better than CT for delineating duct integrity. Contusions (Grade I/II) without duct injury → conservative
Bowel & Peritoneal
Condition
Key MRI Findings
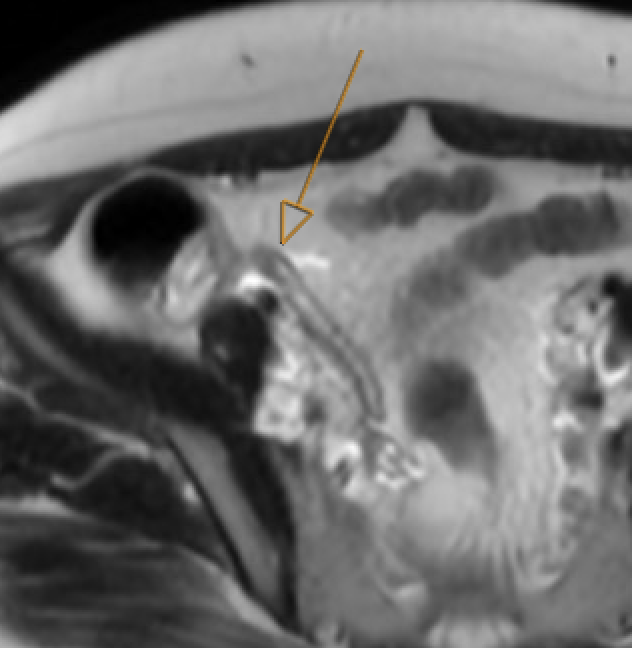
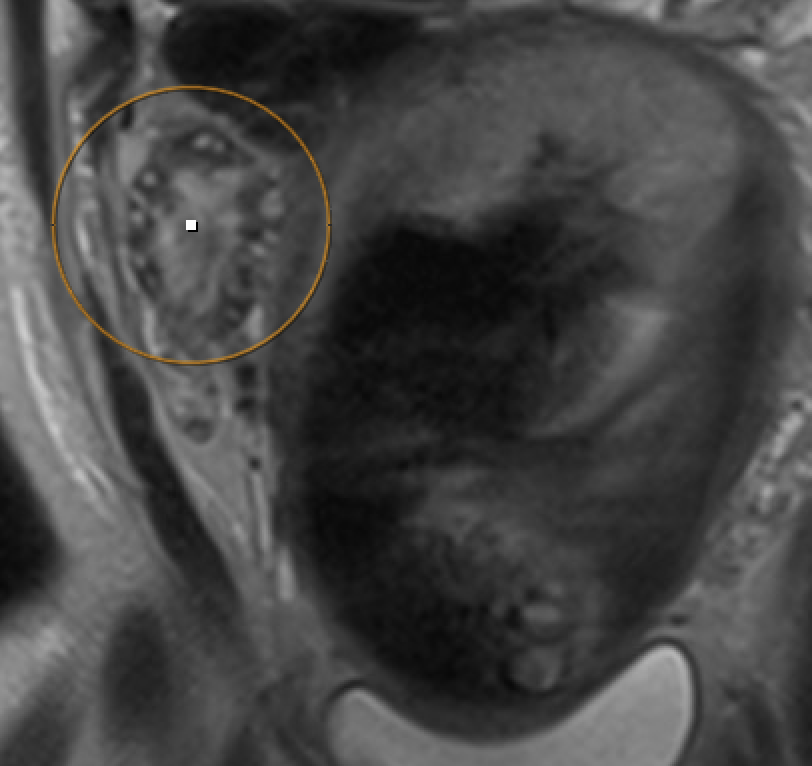
Appendicitis (pregnancy)
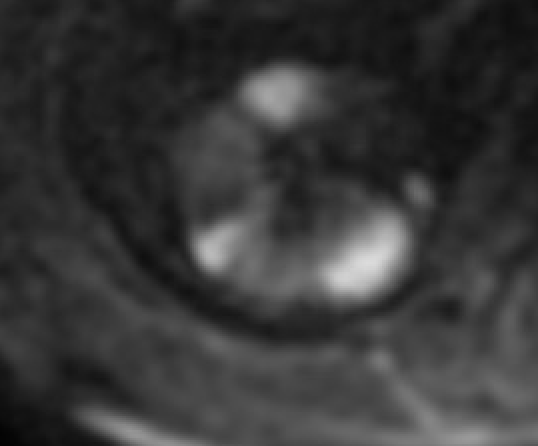
Dilated appendix ≥7 mm, wall thickness >2 mm, periappendiceal fluid/fat stranding on T2W. Appendicolith: T2-hypointense filling defect (confirm on bSSFP). Appendix migrates cranially with gestational age. Sensitivity 94%, specificity 97%
Appendicitis: dilated appendix, periappendiceal stranding
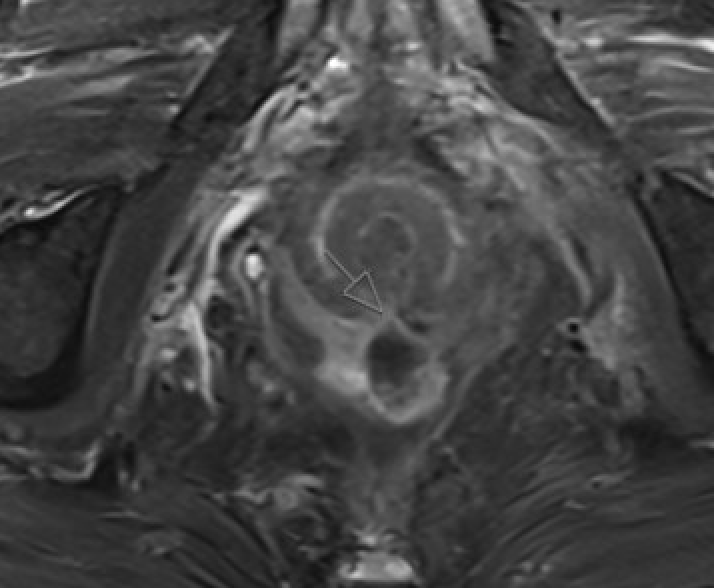
Diverticulitis
Colonic wall thickening >3 mm with diverticula; pericolic fat stranding on T2W FS; abscess: rim-enhancing + DWI-restricting collection. MRI sensitivity 86–94%, specificity 88–92%. Better soft-tissue resolution for fistula, oophoritis
Diverticulitis: wall thickening, pericolic T2 stranding
Crohn complications
Stricture: wall thickening >3 mm + luminal narrowing >50% + upstream dilatation. Penetrating: sinus tract, fistula, phlegmon, abscess (rim enhancement + DWI restriction). Active inflammation: wall edema + hyperenhancement on T2W FS and post-Gd
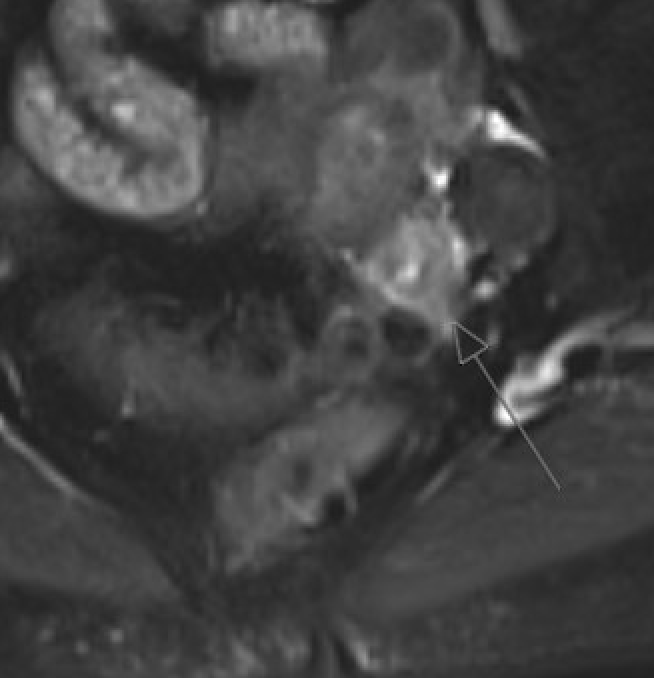
Small-FOV T2W FSE along anal canal is key. Report: tract type (Parks classification — intersphincteric / transsphincteric / suprasphincteric / extrasphincteric), internal and external openings, branches, abscess. DWI + post-Gd for abscess vs granulation vs fibrosis
Perianal fistula: T2W tract, internal opening, sphincter relation
Pneumoperitoneum
Subtle T2-hypointense foci in peritoneal cavity. Air-fluid levels. Susceptibility artifact on bSSFP and T1W GRE sequences. Can be easily missed — look for abnormal extraenteric T2-dark foci
Pneumoperitoneum: T2-dark extraenteric foci, GRE susceptibility
Wedge-shaped nonenhancement with cortical rim sign (preserved capsular vessel enhancement); cortical DWI restriction
Renal infarct: wedge-shaped nonenhancementDelayed: cortical rim sign
Urolithiasis (pregnancy)
Hypointense filling defect in dilated ureter — better seen on bSSFP than T2W. Distinguish from physiologic hydroureteronephrosis (gradual tapering at pelvic brim, right > left)
Subcapsular/perirenal T1-hyperintense collection with T2 signal heterogeneity. Subtraction images mandatory to exclude underlying enhancing neoplasm (AML, RCC most common causes)
OB/GYN Emergencies
Condition
Key MRI Findings
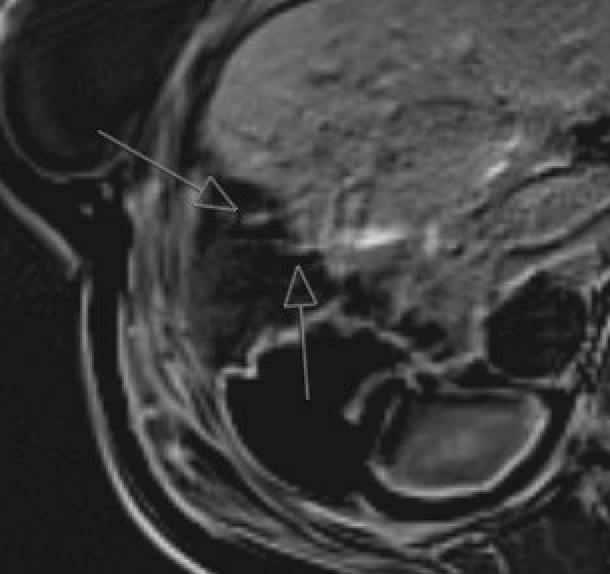
Placental abruption
Retroplacental or subchorionic hematoma: T1-hyperintense blood products (T1 better than T2 for hemorrhage detection). T2 can underestimate hemorrhage extent. bSSFP may show subchorionic hematoma better than T2
Ectopic pregnancy
Gestational sac outside endometrial cavity on T2W. Locations: tubal (most common), cornual, cervical, cesarean scar. MRI localizes ectopic precisely when US is indeterminate. Cesarean scar ectopic: sac in lower uterine segment scar, residual myometrium <2 mm = rupture risk
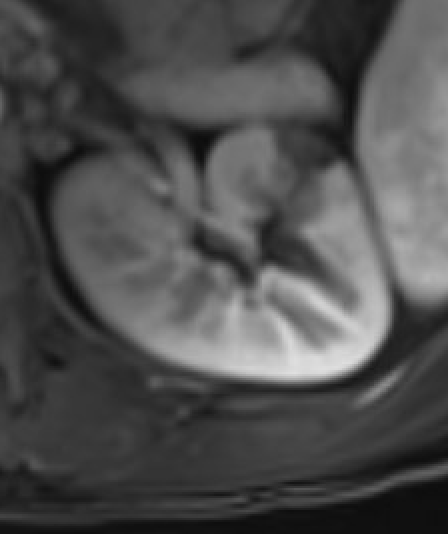
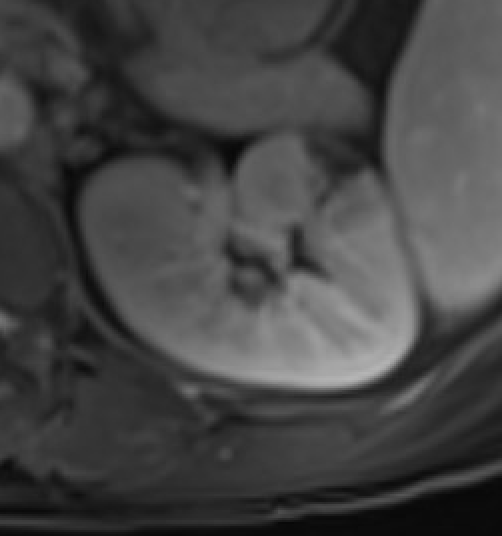
Ovarian torsion (pregnancy)
Enlarged ovary with peripheral follicles and stromal edema on T2W. Pelvic ascites. Compare with contralateral ovary. Whirlpool sign of twisted pedicle
Ovarian torsion: enlarged ovary, peripheral follicles, stromal edema
Postpartum hemorrhage — RPOC vs UVA
RPOC: enhancing endometrial tissue (≤ myometrium = moderate; > myometrium = hypervascular). Serial β-hCG decreases. UVA/AVF: serpiginous flow voids, early draining vein on time-resolved MRA. Low-flow UVA: myometrial blush without early draining vein
MRI in pregnancy — key principles: Safe at ≤3 T (prefer 1.5 T in 1st trimester). GBCAs are FDA Class C — avoid unless benefit clearly outweighs risk; use lowest dose of macrocyclic Group II GBCA with informed consent. Non-contrast sequences (T2W SSFSE, DWI, bSSFP, T1W) are sufficient for most acute indications. For renal failure (eGFR <15): Group II GBCAs can be used after risk-benefit discussion; space injections ≥7 days apart.
📄Panda A, Aswani Y, Heming CAM, et al. On-Call Body MRI: A Primer. RadioGraphics. 2025;45(1).