Indications & Patient Selection
Indications
- Axial low back pain with SI joint origin — duration ≥3 months, failed conservative therapy (NSAIDs, physical therapy, sacral belting)
- SI joint pain characteristics: pain below L5, buttock pain, PSIS tenderness, groin pain; worsened with single-leg stance; Gaenslen test positive; FABER (Patrick) test positive
- Sacroiliitis: ankylosing spondylitis, psoriatic arthritis, reactive arthritis, post-partum SI dysfunction, post-lumbar fusion SI stress
- Diagnostic injection: ≥50% pain relief after intra-articular steroid/anesthetic confirms SI joint etiology
- Post-fusion SI pain: up to 40% of patients develop SI joint pain within 5 years of lumbar fusion — low threshold for injection in this population
Contraindications & Workup
- Absolute contraindications: Active infection over injection site · Uncorrectable coagulopathy · Pregnancy · Allergy to contrast or corticosteroids
- MRI pelvis: evaluate for sacroiliitis, subchondral erosions, bone marrow edema (STIR sequences), bridging or ankylosis
- X-ray SI joint: sclerosis, joint space changes, bridging osteophytes
- ESR / CRP: elevated in inflammatory arthropathy (ankylosing spondylitis, psoriatic arthritis)
- HLA-B27: obtain if ankylosing spondylitis suspected — guides long-term management and biologic therapy referral
Pre-Procedure Checklist
Relevant Anatomy
SI Joint Structure
- Diarthrodial synovial joint (anterior inferior portion) — true joint with hyaline and fibrocartilage, synovial lining in the lower 2/3, and thick fibrous capsule
- Posterior syndesmosis — fibrocartilaginous/ligamentous component (dorsal, interosseous, iliolumbar ligaments); primary stability source
- Joint space: 2–4 mm; irregular margins; widest inferiorly — the inferior joint is the primary injection target
- Joint capacity: ~2–2.5 mL; overfilling causes periarticular extravasation and reduces efficacy
- Synovial lining in lower 2/3 renders it susceptible to inflammatory arthropathies (ankylosing spondylitis, psoriatic arthritis)
Innervation & Nearby Structures
- Innervation: L4–S3 dorsal rami (posterior SI ligament) + sacral plexus branches (anterior capsule); explains why lateral branch RFA at L4–S3 is effective
- Key target landmark: posterior inferior joint line at S3–S4 level — most accessible entry point on oblique fluoroscopy
- Sacral foramina (S1–S4): medial to joint; inadvertent foraminal injection causes nerve root irritation — the critical error to avoid
- Sciatic notch: inferior and lateral — avoid
- Iliac vessels: anterior to joint — relevant for anterior approaches; use CT if anterior access required
- Fluoroscopic challenge: oblique joint orientation + overlapping iliac and sacral cortices → ipsilateral oblique view mandatory to separate joint lines
Technique
Default RadCall approach · share your own below
Supplies
Steps
Position & AP fluoroscopy
Ipsilateral oblique view
Target the inferior joint margin
Advance needle to posterior joint line
Arthrogram confirmation
Inject therapeutic mixture
Withdraw & recover
For patients with predominantly posterior ligamentous SI pain (rather than intra-articular). Also consider when intra-articular access is obstructed by ankylosis.
Target posterior SI ligament
Inject periarticular
If repeated injections provide only temporary relief (<3 months per injection), refer for lateral branch radiofrequency ablation of L4–S3 dorsal rami. This is a separate procedure targeting the nerve supply to the posterior SI ligament and joint capsule. Escalate to RFA after 3 injections with inadequate duration of relief.
Fluoroscopic Landmarks
View-by-View Guide
- AP view: SI joint appears as 2–3 overlapping lines due to the oblique joint orientation and superimposed iliac/sacral cortices. Not adequate for needle guidance alone.
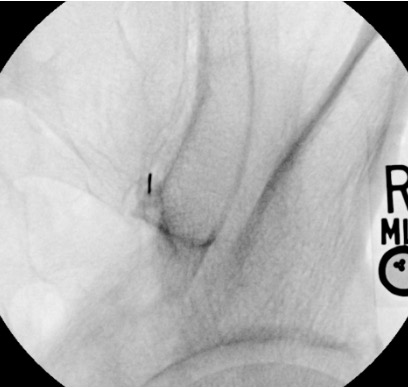
- Ipsilateral oblique (15–25°): Separates the joint into a single clear lucent line. The inferior portion is most accessible. This is the primary working view for needle advancement.
- Lateral view: Useful to confirm needle depth at the posterior joint line. Tip should project at the posterior margin of the joint, not through to the anterior compartment.
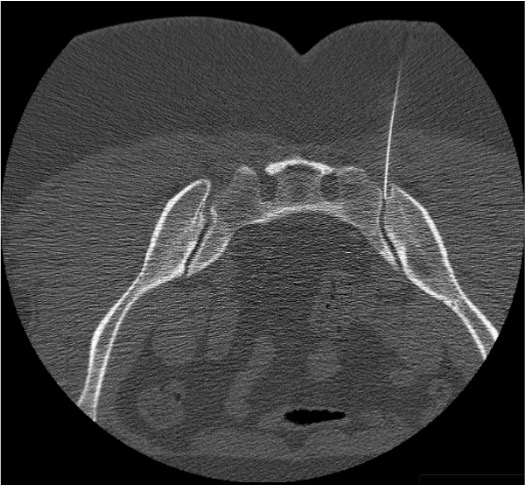
- CT guidance: Preferred when ankylosis is present (ankylosing spondylitis) or when the joint is not well visualized fluoroscopically. Allows direct visualization of needle tip in the joint space.
Arthrogram Interpretation
- Correct intra-articular: Contrast fills the inferior joint pouch; linear tracking along the posterior joint margin; gradual spread within the irregular joint contours
- Foraminal injection (too medial): Contrast flows into S1–S4 foramina — linear contrast extending medially from the sacral side; STOP, withdraw, redirect laterally
- Intra-osseous position: "Bone blush" — diffuse opacification of cancellous bone without joint space filling; STOP, withdraw, redirect
- Vascular uptake: Linear streaming contrast disappearing rapidly; STOP and reposition before injecting steroid
- Periarticular spread only: Diffuse pooling around joint without joint cavity filling; may still be therapeutic for ligamentous pain (periarticular injection)
Troubleshooting
Needle does not enter the joint
Likely cause: Starting point too superior; insufficient oblique angulation; tough posterior ligament in older or ankylosed patients.
Next step: Try a more inferior starting point — the inferior 1/3 of the joint is widest and most accessible. Increase oblique angulation to 25°. If ligament is very tough, upsize to 20G needle. Consider CT guidance if fluoroscopic access remains difficult.
Contrast flows into sacral foramen
Likely cause: Needle tip too medial — sitting in or adjacent to S1–S4 foramen on the sacral side of the joint.
Next step: Withdraw needle and redirect laterally. On the oblique view, target the middle or lateral aspect of the inferior joint line rather than the medial margin. Reconfirm arthrogram before injecting steroid.
Pain with injection / intra-osseous needle
Likely cause: Needle tip within sacral or iliac cancellous bone. Contrast will show a "bone blush" — diffuse opacification of bone without joint cavity filling. Patient typically reports sharp, deep aching pain with injection.
Next step: STOP injecting. Withdraw needle 2–3 mm and reconfirm with small contrast injection. If arthrogram confirms joint entry, proceed. If still intra-osseous, withdraw fully and reposition.
Only extra-articular spread on arthrogram
Likely cause: Needle is periarticular rather than intra-articular. Patient may have predominantly ligamentous SI pain rather than pure intra-articular disease. Also seen in partially ankylosed joints.
Next step: Periarticular injection is still therapeutic for posterior ligamentous SI pain. Proceed with injection of 1–2 mL steroid/anesthetic into the periarticular tissues. Document that injection was periarticular — this affects interpretation of diagnostic utility (articular vs. ligamentous etiology).
Complications
Immediate / Periprocedural
- Post-injection flare (10–20%) — transient pain increase 24–48h post-injection; resolves with NSAIDs and ice; warn patient before discharge; does not indicate failed procedure
- Intra-foraminal injection with nerve injury — rare with fluoroscopic guidance and arthrogram confirmation; presents as acute radiculopathy; avoid by redirecting laterally when foraminal contrast spread is seen
- Vascular injection — risk primarily with anterior approach without CT guidance (proximity to iliac vessels); use posterior fluoroscopic approach routinely
- Vasovagal reaction — manage with supine positioning, IV fluids, atropine if needed
Delayed
- Septic sacroiliitis (<0.1%) — fever, escalating joint pain, elevated WBC/CRP; MRI with contrast for diagnosis; broad-spectrum IV antibiotics; IR or surgical drainage if abscess forms; strict sterile technique prevents this
- Steroid side effects: glucose elevation (diabetics — monitor 24–48h), facial flushing (transient, 24–48h), adrenal suppression with repeated use (limit to 3 per region per year), skin/subcutaneous atrophy from superficial deposition
- Hematoma — rare in Category 1 procedure; usually self-limited; standard anticoagulation hold minimizes risk
Critical Pearls
Community Cards
Institutional and personal technique variations
References
Citations
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology: A Case-Based Approach. Thieme; 2024. Ch. 25 (Dalili D, Dalili DE, Isaac A, Fritz J).
- Rupert MP, Lee M, Manchikanti L, Datta S, Cohen SP. Evaluation of sacroiliac joint injection methods: systematic review. Pain Physician. 2009;12(2):399–404.
- Simopoulos TT, Manchikanti L, Gupta S, et al. Systematic review of the diagnostic accuracy and therapeutic effectiveness of sacroiliac joint interventions. Pain Physician. 2015;18(5):E713–E756.
- Zheng P, Schneider BJ, Yang A, McCormick ZL. Image-guided sacroiliac joint injections: an evidence-based review of best practices and clinical outcomes. PM R. 2019;11 Suppl 1:S98–S104.
- Foley BS, Buschbacher RM. Sacroiliac joint pain: anatomy, biomechanics, diagnosis, and treatment. Am J Phys Med Rehabil. 2006;85(12):997–1006.
- SIR Standards of Practice Committee. Consensus Guidelines for Periprocedural Management of Coagulation Status. J Vasc Interv Radiol. 2012;23(6):727–736.
References & Resources
Key Guidelines
- ISIS Practice Guidelines for SI Joint Procedures
- ASIPP Evidence-Based Guidelines for SI Joint Interventions
- ACR Appropriateness Criteria for Low Back Pain
Primary References
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology. Thieme; 2024. Ch. 25: SI Joint Injection.
- Manchikanti L et al. An update of comprehensive evidence-based guidelines for interventional techniques in chronic spinal pain. Pain Physician. 2013;16(2 Suppl):S49-283.
- Cohen SP. Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment. Anesth Analg. 2005;101(5):1440-1453.