Indications & Patient Selection
Indications
- Refractory sciatica (failed conservative management + epidural steroid injections)
- Oncologic pain in sciatic distribution: pelvic tumor directly involving or compressing sciatic nerve (colorectal, endometrial, sarcoma, sacral metastasis)
- Post-amputation phantom limb pain — cryoneurolysis of residual limb sciatic nerve
- Piriformis syndrome — sciatic nerve compression by hypertrophied piriformis; piriformis injection/Botox as first step; perisciatic injection as adjunct
- Diagnostic nerve block before cryoablation to confirm target
- Palliative pain control in terminal cancer with intractable sciatic-distribution pain refractory to opioids
Contraindications
- Uncorrectable coagulopathy
- Pre-existing complete sciatic nerve injury (no diagnostic value; ablation may worsen functional outcome)
- Patients requiring immediate full ambulation post-procedure (complete motor block expected — foot drop for 6–12 h after block, weeks after cryo)
- Active gluteal/sciatic soft tissue infection
- Negative diagnostic block (cryoablation will not provide benefit)
Block vs. Cryoablation vs. Piriformis Injection
| Indication | Preferred Approach | Notes |
|---|---|---|
| Diagnostic / first-line therapeutic | Perisciatic block (bupivacaine ± steroid) | Confirms sciatic distribution; assess motor effect before ablation |
| Piriformis syndrome | Piriformis intramuscular injection (Botox ± bupivacaine) | Target piriformis muscle bulk, not sciatic nerve; Botox 50–100 units + 10 mL LA |
| Refractory benign sciatica / phantom limb | Cryoablation (perisciatic, subgluteal) | Reversible; nerve regeneration 6–8 wks; preferred over chemical neurolysis |
| Oncologic pain (unresectable tumor) | Cryoablation ± chemical neurolysis | Longer-acting for limited life expectancy; discuss motor deficit expectations |
Pre-Procedure Planning
Imaging
- MRI pelvis/lumbar spine — characterize nerve compression source; rule out disc herniation or central canal stenosis amenable to neurosurgery
- MR neurography if available — assess sciatic nerve signal and caliber; T2 hyperintensity = active inflammation/injury
- CT pelvis for planning — visualize greater trochanter, ischial tuberosity, subgluteal space geometry
- For oncologic cases: recent CT or PET-CT to document tumor extent and nerve involvement
Assessment & Labs
- Baseline neurologic exam: document motor strength (hip flexion, knee extension, dorsiflexion, plantar flexion) and sensory distribution before procedure
- Nerve conduction velocity (NCV) / EMG for complex or post-surgical cases
- INR, platelet count (SIR Cat 1: INR ≤2.5, plt ≥25K)
- Fall risk assessment — physical therapy consult for high-risk patients before cryoablation
- AFO brace procurement for cryoablation cases (expected foot drop)
Anatomy
Nerve Origin & Course
- Largest nerve in the body; formed from L4–S3 nerve roots of the lumbosacral plexus
- Exits pelvis through greater sciatic foramen, below piriformis muscle (piriformis variant: nerve passes through or above piriformis — seen in ~15%)
- Subgluteal space: runs between greater trochanter (lateral) and ischial tuberosity (medial) under gluteus maximus — optimal CT-guided access point
- Descends in posterior thigh; divides into tibial nerve (medial) and common peroneal nerve (lateral) at popliteal fossa
- Posterior femoral cutaneous nerve (PFCN) runs alongside sciatic in subgluteal space — may be co-blocked; fat plane between PFCN and ischial tuberosity is distinct target
CT Landmarks & Motor Distribution
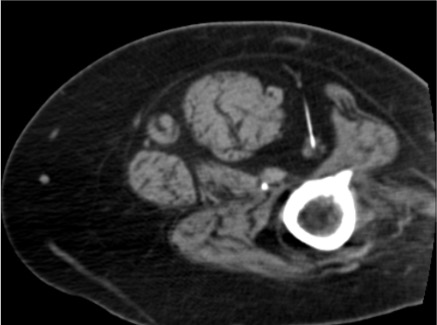
- Subgluteal approach: needle targets perineural fat between greater trochanter (lateral) and ischial tuberosity (medial), posterolateral to sciatic nerve
- Sciatic nerve appears as elliptical structure with internal fascicular architecture (fascicles visible on CT) in the perisciatic fat
- Tibial division: plantar flexion, toe flexion, posterior leg sensation
- Common peroneal division: dorsiflexion, eversion — foot drop if injured/blocked
- Proximal approach (ischial spine level): larger nerve cross-section; more predictable spread; used for oncologic or high-level entrapment
Technique
CT-Guided Subgluteal Approach (Block)
Positioning & CT Planning
Skin Prep & Local Anesthesia
Needle Advancement to Perisciatic Fat
Intraneural Check + Aspiration
Contrast Injection Test
Medication Injection
Post-Injection Motor Exam
Piriformis Injection Variant
Target Piriformis Muscle Belly
Cryoablation Variant (After Positive Diagnostic Block)
17G Cryoprobe Placement
Freeze-Thaw-Freeze Protocol
Ice Ball Monitoring
Active Thaw & Probe Removal
Community Cards
Troubleshooting
Intraneural Placement
Sharp radiating pain to leg on needle advancement or injection = intraneural. Withdraw immediately 2–3 mm without injecting. Reconfirm position on CT — needle tip should be in perineural fat plane. If resistance to injection felt: intraneural; stop and reposition before proceeding.
Intravascular Injection
Aspiration of blood or rapid washout of contrast on CT test → reposition. Gluteal artery or sciatic vascular bundle can be adjacent. If systemic symptoms develop after injection (metallic taste, tinnitus, cardiovascular instability): intravascular local anesthetic — resuscitation protocol; no further injection at this site.
Block at Ischial Tuberosity Not Effective
If subgluteal block provides incomplete or no relief: consider piriformis syndrome — nerve compression above subgluteal space. Target piriformis muscle with Botox injection at greater sciatic notch level. Alternatively, target nerve more proximally at ischial spine/sciatic notch level.
Ice Ball Not Adequately Covering Nerve
On CT monitoring: ice ball offset or insufficient. Active thaw and reposition probe parallel to nerve course — longer probe positioning allows longer ice ball. Second probe placed 1 cm from first creates larger confluent ablation zone. Confirm both probes in perineural fat before resuming freeze.
Complications
Expected / Predictable Effects
- Foot drop (complete motor block) — expected with any perisciatic intervention; block lasts 4–12 h; cryoablation motor deficit lasts weeks; resolves as nerve regenerates at 1–2 mm/day
- Posterior thigh numbness — expected; may include PFCN distribution
- Transient leg weakness beyond foot drop — hip flexion, knee flexion may be affected
- Post-cryoablation pain flare (days 1–3) — inflammatory reaction; manage with NSAIDs; counsel patient before procedure
Complications
- Gluteal hematoma — most self-limited; compression if superficial; serial CT if expanding; transfuse if Hgb <8
- Infection / abscess — rare; antibiotics; CT-guided drainage if organized
- Neuritis / dysesthesia — partial ablation risk; burning, allodynia; manages with gabapentin; resolves over weeks to months
- Incomplete block with rebound pain exacerbation — acute worsening of symptoms immediately post-cryoablation (before Wallerian degeneration completes); manage with PCA ± hospital admission; resolves within 24 h typically
- Falls / injury — motor block makes ambulation unsafe; document fall risk and provide mobility aids before discharge
Post-Procedure Care
Immediate Recovery
- Motor exam: test dorsiflexion and plantar flexion before any weight-bearing or transfer
- Complete foot drop: patient must not ambulate unassisted — AFO brace and walker/crutches required
- Observe 2 h post-procedure (block: 1 h minimum; cryoablation: 2–4 h)
- Vital signs monitoring; hematoma check at probe sites (cryoablation)
- No driving until motor function confirmed fully returned
Cryoablation Recovery Period
- Warn patient: post-procedure pain exacerbation in first 24 h is common and expected (inflammatory response)
- Nerve regeneration: 1–2 mm/day; most patients recover motor function in 6–8 weeks (epineurium intact preserves regeneration pathway)
- PT/OT referral: exercises to maintain joint range of motion during denervation period; functional electrical stimulation for foot drop
- AFO brace for safe ambulation during recovery
- Gabapentin 300 mg TID if neuritis or dysesthesia
- Ibuprofen 600 mg TID × 5 days for post-cryoablation inflammation
Follow-up Schedule
| Timepoint | Assessment | Action |
|---|---|---|
| 24–48 h | Phone check — post-cryoablation pain flare | Pain control adjustment; confirm safe ambulation; PCA if admitted |
| 2 weeks | Clinic visit — pain diary review, motor exam | VAS score; document motor recovery; PT progress |
| 6 weeks | Full motor/sensory re-exam | Confirm nerve regeneration underway; reassess need for AFO |
| 3 months | Outcome assessment | If pain returns: cryoablation can be safely repeated (epineurium intact) |
Pearls & Pitfalls
Technique Pearls
Critical Pitfalls
References & Resources
Primary References
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology: A Case-Based Approach. Thieme; 2024. DOI: 10.1055/b000000387
- Tran DQ, et al. Cryoneurolysis: a scoping review of the evidence. Reg Anesth Pain Med. 2021;46(3):255–263.
- Prologo JD, et al. Natural history of mixed and motor nerve cryoablation in humans — a cohort analysis. J Vasc Interv Radiol. 2020;31(6):912–916.
- Pezeshk P, Wadhwa V, Chhabra A. CT-Guided Peripheral Nerve Blocks. Chapter 31 in: Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology. Thieme; 2024.
- Kurup AN, et al. Neuroanatomic considerations in percutaneous tumor ablation. Radiographics. 2013;33(4):1195–1215.
References & Resources
Key Guidelines
- ASRA Practice Guidelines for Regional Anesthesia
- ISIS Guidelines for Peripheral Nerve Blocks
Primary References
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology. Thieme; 2024.
- Peng PW, Narouze S. Ultrasound-guided interventional procedures in pain medicine: a review of anatomy, sonoanatomy, and procedures. Reg Anesth Pain Med. 2009;34(5):458-474.
- Neal JM et al. ASRA Practice Advisory on Neurologic Complications in Regional Anesthesia. Reg Anesth Pain Med. 2015;40(5):401-430.