Indications & Patient Selection
Indications
- Pelvic Congestion Syndrome (PCS): chronic pelvic pain (≥6 months) caused by pelvic varicosities from ovarian vein and/or internal iliac vein incompetence
- Demographics: multiparous women aged 20–45 years; dilated pelvic veins (ovarian vein >5 mm, pelvic varicosities >4 mm)
- Classic symptoms: dull aching pelvic pain worsened by prolonged standing/sitting, after intercourse (dyspareunia), and premenstrually; characteristically relieved by lying down
- Associated findings: vulvar varicosities, left flank/leg varicosities
- Diagnosis: pelvic US with duplex for reflux; MRI/MRV pelvis; catheter venography (gold standard); Valsalva maneuver uncovers reflux on static imaging
- Workup before referral: gynecology consultation to exclude endometriosis, ovarian cysts, and PID; VAS pelvic pain score; sexual/functional impact assessment
Contraindications
- Absolute: Active pelvic infection · Pregnancy · Severe uncorrectable coagulopathy · IVC thrombosis or atresia precluding venous access
- Relative: Postmenopausal (PCS less likely; pain frequently subsides after menopause) · No hemodynamic reflux demonstrated on venography (do not embolize anatomically dilated veins without confirmed reflux)
- Note: Dilated pelvic veins on imaging are not sufficient for treatment — hemodynamic reflux must be confirmed at catheter venography before embolization
Pre-Procedure Checklist
Relevant Anatomy
Ovarian Vein Drainage
- Left ovarian vein: drains into the left renal vein at a right angle; longer course than the right; higher reflux rate because absence of valves is found in 13–15% of women on the left vs. 6% on the right
- Right ovarian vein: drains directly into the IVC on the right lateral wall at an oblique angle; smaller ostium; less commonly incompetent but significant reflux occurs in ~41% of symptomatic patients
- Valvular incompetence: reflux occurs in 43% of symptomatic patients; 31% left, 41% right (Ahlberg et al.)
- Pregnancy effect: hormonal changes cause massive dilation up to 60x normal diameter; significant distention may persist 6 months postpartum and worsen with subsequent gestations
Pelvic Varicosity Distribution
- Reflux pathway: ovarian vein reflux → broad ligament veins → parametrial, uterine, and vaginal varicosities; cross-filling to contralateral pelvis is common
- Internal iliac tributaries: uterine and vaginal branches of bilateral internal iliac veins are a second independent source of reflux; must be assessed and treated if contributing
- Vulvar and leg varicosities: pelvic varicosities may extend to vulva and upper thigh; these typically regress after ovarian vein embolization within 2–3 months
- Venographic diagnosis criteria: tortuous pelvic vein >4 mm diameter, poor flow (<3 cm/s), distended communicating veins, retrograde filling on Valsalva
Nutcracker Syndrome (Secondary PCS)
- Mechanism: compression of the left renal vein between the superior mesenteric artery (SMA) and aorta → left renal venous hypertension → retrograde flow into left ovarian vein → secondary valvular incompetence
- Recognition: LRV diameter <6 mm at the aorto-mesenteric segment; pressure gradient >3 mmHg across compression; contrast reflux into left ovarian vein seen spontaneously without Valsalva
- Treatment implication: if LRV compression is severe, stenting the left renal vein may be the definitive treatment rather than ovarian vein embolization alone; ovarian vein embolization alone may not control reflux if the underlying venous hypertension persists
- Anatomy diagram concept: Left ovarian vein takeoff from LRV → descends in retroperitoneum → enters pelvic basin → broad ligament varicosity plexus → cross-fills contralateral parametrial and uterine veins
Technique
Default RadCall approach · share your own below
Supplies
Steps
Vascular access
Left renal vein catheterization and nutcracker assessment
Left ovarian vein cannulation and diagnostic venogram
Microcatheter placement to distal varicosity plexus
Sclerosant foam embolization of varicosity plexus
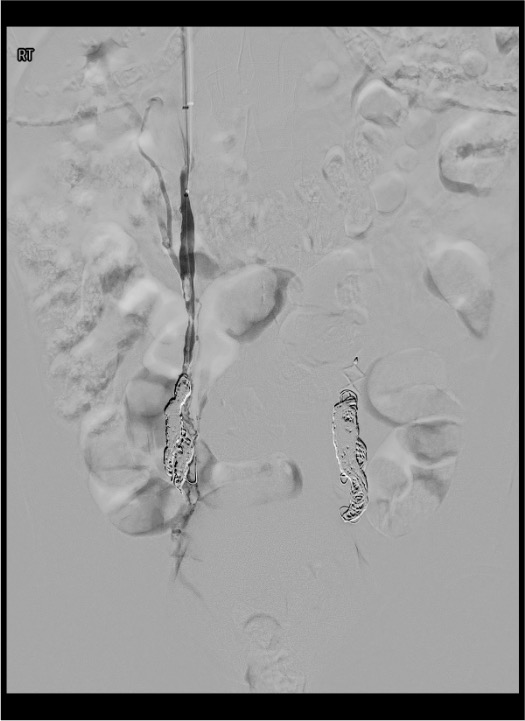
Coil embolization — distal to proximal

Right ovarian vein assessment and embolization
Internal iliac vein assessment
Final venogram and hemostasis
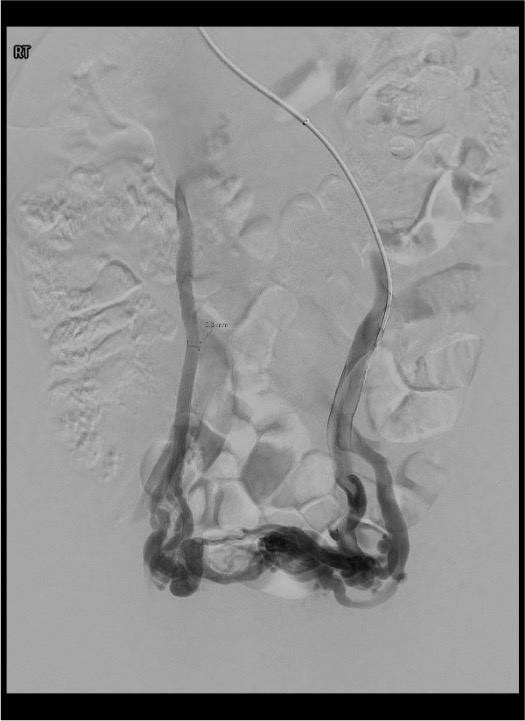
Venographic Landmarks
Left Ovarian Vein
- Takeoff from LRV: gooseneck angulation at the LRV-LOV junction; best approached coaxially from RIJ; catheter should point inferiorly to engage the ostium
- Diameter: 5–8 mm with reflux; normal is <5 mm
- Reflux pattern: contrast flows retrograde into broad ligament and parametrial plexus during Valsalva or spontaneously in severe cases
- Nutcracker sign: spontaneous reflux into left ovarian vein during LRV injection without Valsalva; LRV diameter <6 mm at aorto-mesenteric segment
Right Ovarian Vein and Internal Iliac Tributaries
- Right ovarian vein takeoff: directly from IVC right lateral wall; oblique/caudal orientation; small ostium; Berenstein or C2 catheter usually required from femoral approach; may be absent or atrophic if not a dominant reflux source
- Internal iliac tributaries: catheterize off bilateral internal iliac veins; uterine and vaginal branches are the most common contributing tributaries; assess if pelvic varicosities are not fully explained by ovarian vein reflux
- Cross-filling pattern: contrast refluxing across midline from left to right pelvis on left ovarian venogram indicates bilateral pelvic involvement
- Pressure gradient: nutcracker confirmed if LRV-IVC pressure gradient >3 mmHg
Venographic Criteria for PCS Diagnosis
| Finding | Threshold | Significance |
|---|---|---|
| Ovarian vein diameter | >5 mm | Suggests incompetence; >8 mm highly specific |
| Pelvic varicosity diameter | >4 mm | Venographic diagnostic criterion (Beard et al.) |
| Pelvic venous flow velocity | <3 cm/s | Poor drainage; venographic criterion for PCS |
| Reflux on Valsalva | Any retrograde flow | Confirms valvular incompetence; embolization indicated |
| Nutcracker gradient | >3 mmHg LRV-IVC | Indicates significant LRV compression; consider stenting |
| Distended communicating veins | Present | Confirms pelvic varicosity plexus; third diagnostic criterion |
Troubleshooting
Cannot catheterize left ovarian vein from LRV
Likely cause: Acute angulation at LRV-LOV junction; small or atrophic ostium; catheter too straight.
Next step: The left renal vein is your guide landmark. Switch to a reverse-curve catheter (RIM or Simmons 1) to engage the downward-oriented left ovarian vein ostium. Have the patient perform a Valsalva maneuver to increase venous pressure and open the ostium. If still unsuccessful from RIJ, attempt from femoral approach with a cobra or reversed catheter configuration.
Right ovarian vein not visualized or not accessible
Likely cause: Right ovarian vein may be very small, atrophic, or not a dominant contributor to pelvic reflux. The IVC ostium can be difficult to engage from femoral approach.
Next step: If no reflux is demonstrated on venography with Valsalva, the right ovarian vein is not a significant contributor — do not embolize. Ensure you have performed an adequate venogram; a Berenstein or C2 catheter from the femoral approach, or a Cobra from the RIJ, improves engagement. If access truly fails but reflux was seen on pre-procedure imaging, note for possible second-session evaluation.
Sclerosant foam migrates centrally toward IVC
Likely cause: Injection volume too large; flow rate in varicosity plexus is brisk and not stagnant; microcatheter not positioned far enough distally.
Next step: Use smaller aliquots (1–2 mL instead of 3–4 mL). Confirm sluggish or stagnant contrast flow in the varicosity before each foam injection. Re-advance microcatheter more distally. Deploy a coil or two proximal to the injection site to slow antegrade flow before foam injection. Stop foam injection immediately if foam is seen tracking centrally.
Pelvic pain not improving at follow-up
Likely cause: Missed internal iliac tributaries contributing to varicosity filling; incomplete bilateral ovarian vein embolization; residual cross-filling from contralateral pelvis.
Next step: Obtain follow-up pelvic US or MRV at 3 months to assess for residual varicosities. If residual disease is present, plan a second session to evaluate and embolize bilateral internal iliac uterine/vaginal tributaries. Confirm right ovarian vein was adequately treated at the initial procedure.
Coil malposition or migration
Likely cause: Coil undersized relative to vein diameter; deployed in a location without adequate landing zone; pushed distally during deployment.
Next step: If coil is in a hemostatic position even if not ideal, assess clinically and consider leaving. If coil has migrated to pulmonary vasculature (check chest radiograph post-procedure), small peripheral coils in distal PA branches may be observed. Large coils or centrally positioned PA coils require snare retrieval in the cardiac catheterization lab. Prevention: size coils 20–30% oversized to vessel diameter.
Complications
Periprocedural / Early (<1 week)
- Post-embolization syndrome (common): pelvic pain, low-grade fever, nausea/vomiting 2–5 days post-procedure; managed with NSAIDs, anti-emetics, and oral hydration; discharge with pain management plan; warn patients this is expected and does not indicate a complication
- Non-target embolization: sciatic nerve, bladder, or bowel injury from foam sclerosant tracking outside the target veins; avoid foam injection when flow is brisk centrally; use small aliquots and confirm stasis before each injection
- Coil migration to pulmonary vasculature: rare; prevent by sizing coils 20–30% oversized; if small coil migrates to distal PA, may observe; central PA migration requires snare retrieval
- Venous access complications: RIJ hematoma, pneumothorax (RIJ access); CFA hematoma (femoral access); standard post-procedure monitoring and hemostasis protocols apply
Delayed / Long-Term
- Recurrence / treatment failure: 20–30% partial recurrence at 2 years; most commonly due to untreated contralateral ovarian vein or internal iliac tributaries; re-treatment with second-session internal iliac embolization often successful
- Ovarian vein thrombophlebitis: very rare; treated with NSAIDs and anticoagulation if significant
- Ovarian failure: theoretical concern only; ovarian blood supply is entirely arterial (ovarian artery); venous embolization has not been associated with ovarian failure or hormonal disruption in published literature
- Outcomes: 70–80% subjective improvement at 1–2 years (Williams & Murphy; Kim HS et al. JVIR 2006); 85% reduction in dyspareunia; mean success rate ~75% across published series (Daniels et al. JVIR 2016)
Critical Pearls
References
Citations
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology: A Case-Based Approach. Thieme; 2024. Chapter 43 (Williams R, Murphy T): Pelvic Congestion Syndrome.
- Kim HS, Malhotra AD, Rowe PC, Lee JM, Venbrux AC. Embolotherapy for pelvic congestion syndrome: long-term results. J Vasc Interv Radiol. 2006;17(2):289–297.
- Daniels JP, Champaneria R, Shah L, Gupta JK, Birch J, Moss JG. Effectiveness of embolization or sclerotherapy of pelvic veins for reducing chronic pelvic pain: a systematic review. J Vasc Interv Radiol. 2016;27(10):1478–1486.
- Tu FF, Hahn D, Steege JF. Pelvic congestion syndrome-associated pelvic pain: a systematic review of diagnosis and management. Obstet Gynecol Surv. 2010;65(5):332–340.
- Beard RW, Highman JH, Pearce S, Reginald PW. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet. 1984;2(8409):946–949.
- Scultetus AH, Villavicencio JL, Gillespie DL. The nutcracker syndrome: its role in the pelvic venous disorders. J Vasc Surg. 2001;34(5):812–819.
- Edwards RD, Robertson IR, MacLean AB, Hemingway AP. Case report: pelvic pain syndrome — successful treatment of a case by ovarian vein embolization. Clin Radiol. 1993;47(6):429–431. (First reported case of bilateral OVE for PCS.)
- Capasso P, Simons C, Trotteur G, Dondelinger RF, Henroteaux D, Gaspard U. Treatment of symptomatic pelvic varices by ovarian vein embolization. Cardiovasc Intervent Radiol. 1997;20(2):107–111.
- Liddle AD, Davies AH. Pelvic congestion syndrome: chronic pelvic pain caused by ovarian and internal iliac varices. Phlebology. 2007;22(3):100–104.
References & Resources
Key Guidelines
- SIR Standards of Practice for Pelvic Vein Embolization
- CIRSE Standards of Practice for PCS Embolization
Primary References
- Kim HS et al. Embolotherapy for pelvic congestion syndrome: long-term results. J Vasc Interv Radiol. 2006;17(2 Pt 1):289-297.
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology. Thieme; 2024. Ch. 43: Pelvic Congestion Syndrome.
- Champaneria R et al. The relationship between pelvic vein incompetence and chronic pelvic pain in women: systematic reviews of diagnosis and treatment effectiveness. Health Technol Assess. 2016;20(5):1-108.