Indications & Contraindications
Indications
- Osteoporotic VCF with >15% height loss — balloon inflation can restore height before cementing; more height gain than vertebroplasty alone
- Fractures where cement containment is desired — cavity created by balloon reduces free cement flow through cancellous bone (lower leak risk than vertebroplasty)
- Acute fractures with burst pattern and intact posterior wall — controlled balloon inflation can reduce fracture; posterior wall must be intact to prevent retropulsed fragment worsening
- Kyphotic deformity — kyphoplasty provides modest kyphosis correction; preferred when sagittal balance restoration is a goal
- All indications for vertebroplasty also apply — osteoporotic, malignant, and traumatic VCFs with pain refractory to conservative management
Contraindications
- Absolute: Posterior wall disruption with retropulsed fragment causing neurologic deficit (surgery preferred) · Active infection · Uncorrectable coagulopathy · PMMA allergy
- Relative: Vertebra plana (>75% height loss) — balloon may not be deployable; consider SpineJack · Spinal instability requiring surgical fixation · Pregnancy
- Note: Burst fractures with posterior wall compromise — balloon inflation may worsen retropulsion. CT mandatory pre-procedure to assess posterior wall. If any doubt: vertebroplasty or SpineJack preferred over balloon
Kyphoplasty vs. Vertebroplasty — Key Differences
- Height restoration: Balloon inflation before cement provides active fracture reduction; vertebroplasty relies on cement pressure alone — minimal height gain
- Cement containment: Balloon creates a defined cavity; high-viscosity cement fills the cavity — lower leak risk compared to vertebroplasty (direct injection into cancellous bone)
- Cost: Kyphoplasty is more expensive (balloon system ~$1,500–3,000 per level vs. ~$200–400 for vertebroplasty)
- Anesthesia: General anesthesia used at many centers for kyphoplasty; vertebroplasty often MAC/local
- Evidence: FREE trial (Wardlaw et al, Lancet 2009) demonstrated superior outcomes for kyphoplasty vs. conservative management. Adjusted survival rate higher for kyphoplasty vs. vertebroplasty in retrospective Medicare data (Edidin et al)
Pre-Procedure Checklist
Relevant Anatomy
Access Approach
- Standard: Bilateral transpedicular — 8–10G Jamshidi/working cannula bilaterally, each to posterior one-third of vertebral body
- Extrapedicular: Used when pedicle too narrow (<4–5 mm), typically above T8
- Unipedicular (curved balloon): Single right pedicle entry — curved nitinol stylet advanced to traverse midline into contralateral hemivertebra, creating bilateral cavity from single access point
- Level range: T4–L5 (same as vertebroplasty); cervical spine kyphoplasty rare
The Posterior Wall — Critical Landmark
- Posterior cortex separates the vertebral body from the spinal canal and posterior elements
- Any fracture line or fragment involving the posterior wall is a warning sign — forced balloon inflation could displace bone into the canal
- On lateral fluoroscopy: confirm balloon tip does not contact or cross the posterior vertebral cortex during inflation
- Balloon inflation should be monitored in real time — stop at any resistance suggesting posterior wall proximity
Balloon Workspace
- Target position: Balloon placed in the central/anterior trabecular bone, posterior to the anterior cortex, anterior to the posterior wall
- Balloon inflation compacts trabecular bone radially and cranio-caudally, reducing the fracture and creating a defined cavity
- Cavity volume correlates with expected cement volume — do not overfill the cavity with cement
- In areas of dense or sclerotic bone (old fractures, post-radiation), the balloon may not fully inflate — partial restoration still beneficial
Technique
Supplies
Standard Bilateral Kyphoplasty Steps
Position & level localization
Bilateral pedicle entry
Create working channel

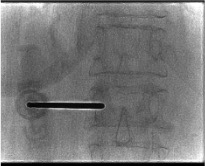
Insert balloons bilaterally
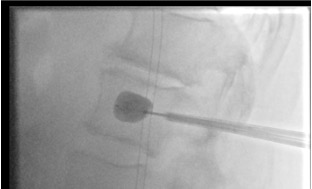
Balloon inflation — height restoration
Balloon deflation & removal
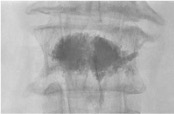
Cement injection into cavity
Needle removal & completion
Curved Balloon Kyphoplasty (AVAflex System)
Single unipedicular access
AVAflex nitinol stylet insertion
Balloon deployment & inflation
Curved needle cement delivery
Troubleshooting
Balloon does not inflate / height not restored
Likely cause: Balloon in dense/sclerotic bone, old fracture with extensive callus, or chronic deformity where trabeculae have remodeled — no reducible fracture cleft remaining.
Next step: Attempt to advance balloon tip into the fracture cleft on lateral fluoroscopy. Try sequential inflation in small increments with increased force. If still no movement: partial inflation may be achievable. Partial height gain with good cavity formation is still clinically beneficial — pain relief does not require complete height restoration. Document outcome and adjust patient expectations.
Cement leak despite cavity — posterior extravasation
Likely cause: Posterior cortical disruption not identified pre-procedure, cement viscosity too low, or overfilling the cavity.
Next step: Stop injection immediately. Wait for cement to polymerize and self-seal at the leak site (1–2 min). Reassess on lateral fluoroscopy. For kyphoplasty, the cavity should contain most cement — leak suggests cortical breach. Abandon injection on that side if leak continues. Post-procedure CT mandatory to characterize extent.
Balloon rupture during inflation
Likely cause: Balloon contacted a sharp bony cortical edge, exceeded maximum inflation volume, or defective balloon.
Next step: Remove ruptured balloon fragments via working cannula (use fluoroscopy to confirm complete removal). Assess whether adequate cavity was created before rupture. If sufficient cavity present: proceed with cement injection. If not: replace with new balloon, or proceed with direct cement injection (converting to vertebroplasty technique). Most balloon remnants are radiopaque and can be confirmed removed on fluoroscopy.
End-plate breakthrough during inflation
Likely cause: Excessive inflation pressure or balloon positioned too cranially/caudally — contacts weakened end plate.
Next step: Stop inflation immediately. Deflate balloon. Reposition to a more central location and reattempt at lower pressure. Minor end-plate breakthrough may result in intradiscal cement leakage during cement injection — monitor carefully and stop if intradiscal filling seen.
Complications
Cement Extravasation (Lower Rate Than Vertebroplasty)
- Epidural: Cord/cauda equina compression — emergent surgical decompression if symptomatic neurologic deficit
- Foraminal: Radiculopathy; usually self-limited
- Intradiscal: End-plate breach leads to intradiscal injection; accelerates disc degeneration
- Venous / PE: Asymptomatic cement PE reported on CT in up to 5%; symptomatic PE rare
- Overall leak rate: Lower than vertebroplasty due to cavity containment — but not zero
Kyphoplasty-Specific Complications
- Failed height restoration: Chronic fractures, sclerotic bone — clinically acceptable if pain relief achieved
- Balloon rupture: Rare; usually manageable (retrieve fragments, proceed)
- End-plate disruption: Balloon inflation may breach end plate; monitor for intradiscal cement
- Adjacent vertebral fracture: As with vertebroplasty — stiffened cemented segment alters biomechanics
- Significant adverse events: 1.0–1.5% in large series (epidural cement requiring decompression, hematoma, osteomyelitis)
Emergent Escalation Triggers
- New neurologic deficit post-procedure → emergent spine surgery consult + CT spine
- Hypoxia / chest pain post-procedure → CT chest angiography (cement PE)
- Severe unremitting pain escalation → CT spine (epidural collection)
Post-Procedure Care
Recovery & Monitoring
- Recover supine 1–2 hours; neurologic exam before discharge
- Ambulate day of procedure when sedation cleared
- Anecdotal pattern: pain relief immediate post-procedure, returns within 24 hours (muscle spasm/inflammation), then resolves over 10–14 days
- Most patients discharged same day (ambulatory procedure) or next morning if admitted
- Post-procedure pain score documentation at 24 hours
Imaging & Follow-up
- Post-procedure CT of treated level to document cement distribution and confirm no canal encroachment
- Upright weight-bearing lateral X-ray at 4–6 week follow-up to assess maintained height restoration (balloon deflation after cement sets ensures durable height)
- Resume anticoagulation: 24 hours post-procedure
- Osteoporosis management referral — bisphosphonates, denosumab, or teriparatide
- Physical therapy for core strengthening and fall prevention
- Counsel on adjacent fracture risk; return to ED for new acute back pain or neurologic symptoms
Critical Pearls
Related Resources
Vertebral Augmentation Comparison
| Feature | Vertebroplasty | Balloon Kyphoplasty | SpineJack |
|---|---|---|---|
| Mechanism | Direct cement injection | Balloon inflation creates cavity, then cement | Titanium implant expands craniocaudally, then cement |
| Height restoration | Minimal | Moderate (balloon inflation before cement) | Superior — up to 40% height gain; durable |
| Cement leak risk | Higher | Lower (contained cavity) | Low (implant contains cement) |
| Sedation | MAC / Local | MAC / General | General / MAC |
| Cost | Lowest | Moderate | Highest |
| Implant remains | No | No (balloon removed) | Yes (titanium implant permanent) |
| Best for | VCF without significant height loss; malignant fractures | Fractures with >15% height loss; intact posterior wall; when cavity containment desired | Acute fractures with significant height loss; young patients; durable restoration |
Primary Reference
Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology: A Case-Based Approach. Thieme; 2024. DOI: 10.1055/b000000387
Chapters 17 (Marshall — Osteoporotic Fracture II: Kyphoplasty) and 19 (McGraw & McGraw — Osteoporotic Fracture IV: Curved Balloon Kyphoplasty)
Additional references: FREE trial — Wardlaw et al, Lancet 2009 · Edidin et al, JBMR 2011 (mortality analysis) · ACR Appropriateness Criteria: VCF Management · SIR Consensus Guidelines for Periprocedural Management · AVAflex FDA approval 2017