Indications & Patient Selection
Indications
- Primary: Knee osteoarthritis (Kellgren-Lawrence grade I–III) with pain ≥4/10 VAS, failed conservative therapy ≥3 months
- Also: Chronic synovitis; post-surgical hemarthrosis or synovitis following knee arthroplasty
- Best candidates: VAS ≥4, KL grade II–III (synovitis/inflammatory component), failed PT + NSAIDs, not yet TKA candidate
- Evidence: Okuno et al — 80% WOMAC improvement at 3 years in KL grade 1–3 patients
Contraindications
- Absolute: Active infection or septic arthritis · Uncorrectable coagulopathy · Severe peripheral vascular disease
- Absolute: Severe CKD (SCr >2.0 or eGFR <30) · Contrast allergy (unpremedicated)
- Relative: End-stage OA (KL grade IV) — inferior results; consider TKA referral
- Relative: Significant atherosclerotic disease of popliteal or tibial vessels
Proposed Mechanism (Angiogenesis Theory)
- VEGF and inflammatory cytokines drive synovial neovascularization → abnormal neovessels provide inflammatory cell access to joint tissues → bone/cartilage destruction and pain
- Perivascular sensory nerve fiber co-growth with neovessels → neuropathic pain contribution (cartilage itself is avascular and has no sensory fibers)
- GAE permanently embolizes these abnormal synovial neovessels → reduces inflammation and interrupts neuropathic pain cycle
- MRI studies confirm significant improvement in synovitis grade 2 years post-GAE (Okuno et al, JVIR 2017)
Pre-Procedure Workup
- Weight-bearing knee X-ray — confirm KL grade and joint space
- CMP, INR/PT — assess renal function and coagulation
- Vascular exam — confirm no significant PVD; consider ABI if concern
- MRI knee (optional but helpful) — confirm synovitis distribution, exclude other pathology
- Informed consent for DSA and embolization
Pre-Procedure Checklist
Relevant Anatomy
Genicular Artery Branches
- Superior Lateral Genicular Artery (SLGA): Arises ~3–5 cm above joint line from popliteal; curves around lateral femoral condyle superiorly
- Superior Medial Genicular Artery (SMGA): Arises ~3–5 cm above joint line; curves around medial femoral condyle
- Inferior Lateral Genicular Artery (ILGA): Arises at or just below joint line; courses below lateral tibial plateau; often multiple small branches
- Inferior Medial Genicular Artery (IMGA): Arises at joint line; courses below medial tibial plateau
- Middle Genicular Artery: Posterior origin; penetrates posterior joint capsule; supplies cruciate ligaments and posterior synovium
- Anterior Tibial Recurrent Artery: From anterior tibial artery; contributes to anterior knee supply
- Descending Genicular Artery: From distal superficial femoral artery; variable contribution
Key Anatomic Considerations

- All genicular arteries arise from the popliteal artery; preserve main popliteal trunk patency throughout procedure
- Target: Branches with abnormal synovial blush (hyperemia/neovascularization); normal articular cartilage receives blood from different vessels not targeted by GAE
- Collateral network: Extensive anastomoses among genicular arteries and with tibial vessels; partial embolization may be offset by collateral reconstitution
- Danger zone: Infrapatellar branches supplying Hoffa fat pad and skin near tibial tubercle — embolization here causes skin necrosis; identify and avoid
- Pain distribution on clinical exam guides target selection — medial pain targets SMGA/IMGA; lateral pain targets SLGA/ILGA
Normal vs. Pathologic Arteriogram
- Normal: Thin, well-defined genicular branches; minimal parenchymal blush in periarticular soft tissues
- OA/synovitis: Markedly increased neovessels; dense, persistent, diffuse synovial blush (hyperemia) — especially in medial and anterior compartments
- Post-arthroplasty hemarthrosis: Focal hypertrophic synovial neovessels, often superomedial distribution
- Compare affected knee arteriogram to published normal anatomy (Fig. 36.4 in source text) — the contrast is striking in symptomatic patients
Technique
Default RadCall approach · share your own below
Supplies
Steps
Arterial access
Navigate to popliteal artery
Popliteal arteriogram — map genicular anatomy
Superselective catheterization with microcatheter
Pre-embolization test injection
Embolize to stasis
Repeat for all hyperemic vessels
Post-embolization popliteal arteriogram
Sheath removal and closure
Treatment Comparison: Knee Pain Options
| Treatment | Best KL Grade | Mechanism | Duration | Notes |
|---|---|---|---|---|
| GAE | I–III | Embolize synovial neovessels; reduce inflammation | Months–years; repeatable | Minimally invasive; ~70–80% responders; skin necrosis risk |
| Genicular Nerve RFA | Any (not surgical) | Ablate sensory genicular nerve branches | 6–12 months; repeatable | Targets pain pathway not source; no effect on synovitis |
| Intra-articular Injection | Any | Corticosteroid anti-inflammation or viscosupplementation | Weeks–months | Max 3–4/year; temporary; limited evidence for viscosupplementation |
| Total Knee Arthroplasty (TKA) | III–IV | Joint replacement | Decades | Definitive for severe disease; major surgery; 15–20 year implant life |
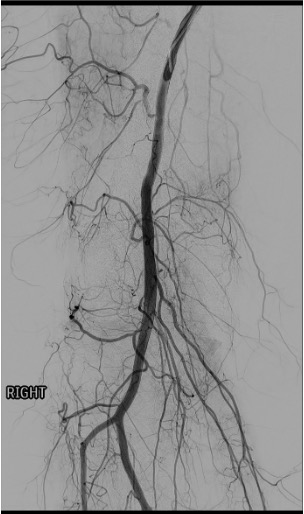
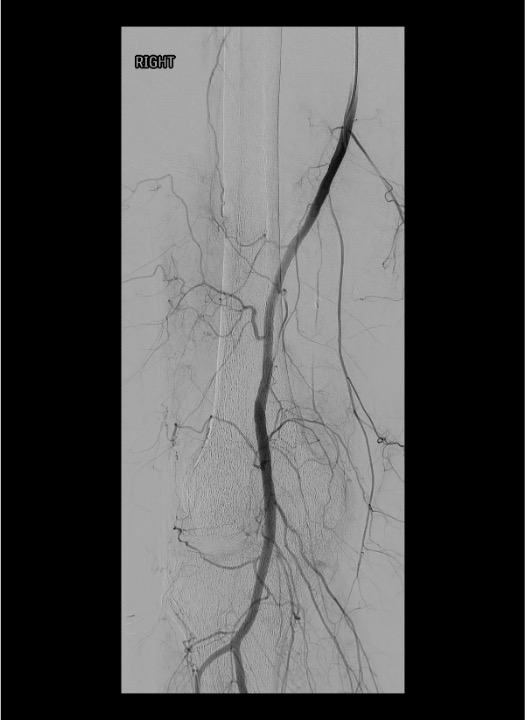
DSA Landmarks & Fluoroscopic Guidance
Vessel Identification on DSA
- Popliteal artery: Centerline vessel in the posterior knee; all geniculars arise from it within ~5 cm above and below joint line
- SMGA / SLGA: Arise 3–5 cm above joint line; curve medially or laterally around respective femoral condyles; visible on AP and oblique views
- IMGA / ILGA: Arise at or just below the joint line; smaller caliber; often multiple branches; best seen on oblique views (30–45°)
- Middle genicular: Short posterior branch; may not be selectively catheterized; contributes less to anterior synovial hyperemia
- Use oblique views (30–45° ipsilateral and contralateral) to separate overlapping vessel takeoffs and open the orifices of individual genicular arteries
Identifying Target vs. Non-Target Blush
- Pathologic synovial blush (target): Persistent, diffuse, hazy enhancement in medial or anterior knee compartment = neovascular hyperemia; inject here
- Normal parenchymal stain: Thin, transient enhancement that clears quickly — not a clear blush
- Skin / subcutaneous blush (danger): Enhancement near tibial tubercle, infrapatellar region, or lateral skin — stop immediately; this is Hoffa fat pad or cutaneous supply; embolization here causes skin necrosis
- Cutaneous branch of popliteal artery: Arises from posterior popliteal; supplies posterior skin; identify and avoid on arteriogram
- Patients may report tingling or pain during injection of target vessels — this is expected and confirms correct positioning
Fluoroscopic Views by Target Vessel
| Target Vessel | Best View | Anatomic Landmark | Key Checkpoint |
|---|---|---|---|
| SMGA | AP + mild ipsilateral oblique | Medial femoral condyle, ~3–5 cm above joint | Confirm medial synovial blush; no skin blush |
| SLGA | AP + contralateral oblique | Lateral femoral condyle, ~3–5 cm above joint | Lateral synovial blush; no peroneal nerve territory blush |
| IMGA | AP + 30–45° ipsilateral oblique | Medial tibial plateau, at joint line | Small vessel; confirm no infrapatellar skin territory |
| ILGA | AP + 30–45° contralateral oblique | Lateral tibial plateau, at joint line | Stop if tibial tubercle/Hoffa blush seen |
Troubleshooting
Cannot catheterize target genicular artery
Likely cause: Unfavorable angle from ipsilateral approach; small caliber vessel; vessel origin obscured by popliteal overlap.
Next step: Switch to contralateral crossover approach — provides a more favorable catheter angle into the popliteal and genicular takeoffs. Try 30–45° oblique views to open the vessel orifice. If vessel is too small for current microcatheter, try a smaller (2.4Fr) or more torqueable system. Roadmap guidance helps navigate tortuous branches.
Skin blush (Hoffa fat pad / infrapatellar) on test injection
Likely cause: Microcatheter has advanced into a branch supplying skin or Hoffa fat pad rather than synovium; most common with ILGA and its infrapatellar branches.
Next step: Do NOT embolize. Pull the microcatheter back slightly and re-test. Look for a synovial blush route that does not communicate with the skin blush territory. If unavoidable, skip this vessel — the risk of skin necrosis outweighs the benefit of embolizing this single branch.
Reflux of embolic particles toward popliteal artery
Likely cause: Injection too fast; forward flow has stalled in the branch and particles are backing up; microcatheter tip too proximal.
Next step: Stop injection immediately. Wait 30–60 seconds for flow to re-establish. Resume with slower injection in 0.1–0.2 mL aliquots. Consider switching to slightly larger particles (100–150 μm) which are less likely to reflux. Advance microcatheter more distally if possible. Never inject with active reflux.
Significant arterial tortuosity preventing microcatheter advancement
Likely cause: Atherosclerotic disease; natural vessel tortuosity at the knee; prior surgery altering anatomy.
Next step: Use the smallest available microcatheter (2.4Fr) with a shapeable microwire. Roadmap guidance throughout. Use a support catheter (5Fr in popliteal) to provide proximal stability. If tortuosity is severe and prevents safe access, skip the vessel and document. Do not force — popliteal injury risk.
Post-procedure synovitis flare (days 1–14)
Expected rate: 10–20% of patients. Increased joint pain, warmth, effusion. Must distinguish from infection.
Next step: Reassure patient — this is expected. Treat with NSAIDs (naproxen 500 mg BID or ibuprofen 600–800 mg TID) for 1–2 weeks. Apply ice. If fever >38.5°C, significant leukocytosis, or disproportionate swelling — aspirate joint to rule out infection. Flare resolves spontaneously in 1–2 weeks and does not predict treatment failure.
Complications
Procedure-Related
- Skin discoloration / necrosis (most feared): Occurs when infrapatellar or cutaneous branches embolized; purple-blue discoloration in 10–15% with Embozene (usually transient); true necrosis rare when technique correct; avoid particles <75 μm and always test inject before embolizing
- Post-embolization syndrome: Low-grade fever, malaise, pain, mild leukocytosis 24–72h post; self-limited; NSAIDs; not infectious
- Tibial / peroneal nerve injury: Rare; risk increased with particles <75 μm; particles ≥75 μm do not reach vasa nervorum of major nerves
- Non-target embolization: Inadvertent popliteal occlusion or tibial vessel involvement; prevented by stasis endpoint (not complete occlusion) and test injection before embolization
Access & Efficacy
- Puncture site hematoma: Standard femoral access complication; manual compression; pseudoaneurysm rare
- Insufficient pain relief (~20–30%): Likely incomplete embolization (missed vessels) or KL IV disease; repeat GAE is feasible; transition to genicular nerve RFA or TKA referral
- Pain recurrence after initial relief: Collateral recruitment or neovessel re-growth; second embolization considered at 6–12 months if recurrence
- Contrast nephropathy: Standard DSA risk; minimize contrast volume; pre-hydrate if borderline renal function; use 50% dilute contrast throughout
Critical Pearls
References
Citations
- Prologo JD, Ray CE Jr., eds. Advanced Pain Management in Interventional Radiology: A Case-Based Approach. Thieme; 2024. Ch. 36: Banathy AK, Sheeran DP, Wilkins LR. Genicular Artery Embolization.
- Bagla S, Piechowiak R, Hartman T, et al. Genicular artery embolization for the treatment of knee pain secondary to osteoarthritis. Cardiovasc Intervent Radiol. 2020;43(7):1019–1028.
- Okuno Y, Korchi AM, Shinjo T, Kato S. Transcatheter arterial embolization as a treatment for medial knee pain in patients with mild to moderate osteoarthritis. Cardiovasc Intervent Radiol. 2015;38(2):336–343.
- Okuno Y, Korchi AM, Shinjo T, Kato S, Kaneko T. Midterm clinical outcomes and MR imaging changes after transcatheter arterial embolization as a treatment for mild to moderate radiographic knee osteoarthritis resistant to conservative treatment. J Vasc Interv Radiol. 2017;28(7):995–1002.
- Landers S, Hely A, Harrison B, et al. Protocol for a single-centre, parallel-arm, randomised controlled superiority trial evaluating the effects of transcatheter arterial embolisation of abnormal knee neovasculature on pain, function and quality of life in people with knee osteoarthritis (GENESIS trial). BMJ Open. 2017;7(5):e014266.
- Little MW, O'Grady A, Briggs J, et al. Genicular Artery embolisation in Patients with Osteoarthritis of the Knee (GENESIS) Using Permanent Microspheres: Long-Term Results. Cardiovasc Intervent Radiol. 2024;47(12):1750–1762. doi:10.1007/s00270-024-03752-7
- Mapp PI, Walsh DA. Mechanisms and targets of angiogenesis and nerve growth in osteoarthritis. Nat Rev Rheumatol. 2012;8(7):390–398.
- Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502.