Indications & Contraindications
Indications
- Massive hemoptysis — >300 mL/24h or any volume causing life-threatening respiratory compromise / asphyxiation risk
- Recurrent hemoptysis — multiple episodes despite conservative management
- Hemoptysis refractory to conservative therapy — failed medical management, bronchoscopic intervention
- BAE is now considered the treatment of choice for massive hemoptysis (surgical mortality 37–43%)
Contraindications
- Absolute: Anterior spinal artery arising from bronchial artery — must identify before embolization; embolization of this vessel causes spinal cord infarction
- Relative: Uncorrectable coagulopathy
- Relative: Contrast allergy (premedicate)
- Relative: Renal insufficiency (minimize contrast)
Common Etiologies
| Category | Etiologies |
|---|---|
| Infectious | Tuberculosis, aspergilloma (mycetoma), lung abscess, necrotizing pneumonia |
| Structural | Bronchiectasis, cystic fibrosis |
| Neoplastic | Lung cancer (primary or metastatic) |
| Other | Cryptogenic (up to 25%), pulmonary arteriovenous malformations, trauma |
Pre-Procedure Planning
Imaging & Labs
- CTA chest — identify bleeding source, bronchial artery anatomy, enlarged/hypertrophied bronchial arteries, look for spinal artery feeders
- CTA accuracy for localizing bronchial artery bleeding approaches 100%; non-bronchial sources ~62%
- Identify variant anatomy: bronchial arteries from subclavian, IMA, thyrocervical trunk
- Labs: CBC, PT/INR, PTT, type & screen
- Review anticoagulation: BAE is SIR Category 2 (moderate risk). Warfarin: hold 5 days (INR <1.5). LMWH: hold 24h. DOACs: hold 24–48h. Aspirin: continue. Clopidogrel: risk-based — often does not need to be held; hold 5 days if bleeding risk exceeds thrombotic risk
Airway Stabilization
- Intubation if massive hemoptysis — protect airway from aspiration/asphyxiation
- Single-lung ventilation (double-lumen ETT or bronchial blocker) to isolate bleeding lung
- Position bleeding side down — prevents blood from flooding unaffected lung
- Bronchoscopy to lateralize bleeding source if CTA not available or indeterminate
- Fluid resuscitation and blood product transfusion as needed
Relevant Anatomy
Bronchial Artery Origins
- ~70% arise from the descending thoracic aorta at T5–T6 level
- Right intercostobronchial trunk (ICBT) — most common configuration; supplies the right bronchial artery + right intercostal artery; typically arises from the right side of the aorta
- Left bronchial arteries — 1–2 arteries, arise from anterior/left aspect of the aorta
- 16–30% of bronchial arteries arise outside T5–T6 (ectopic origins)
Variant Origins
- Subclavian artery
- Internal mammary artery (IMA)
- Thyrocervical trunk
- Costocervical trunk
- Brachiocephalic artery
- Inferior phrenic artery
- Abdominal aorta / aortic arch
CRITICAL — Anterior Spinal Artery
- The anterior spinal artery can arise from a bronchial artery or intercostal artery — embolization causes spinal cord infarction and paralysis
- Look for the characteristic “hairpin” loop on selective angiography — a small branch coursing medially toward the spinal canal with a sharp turn
- If spinal artery is visualized: ABORT embolization of that vessel. Use microcatheter to achieve more distal purchase beyond the spinal artery origin, or abandon that artery entirely.
- Provocative testing with intra-arterial lidocaine or short-acting barbiturate can detect occult spinal artery supply
Technique
Vascular Access
Descending Thoracic Aortogram
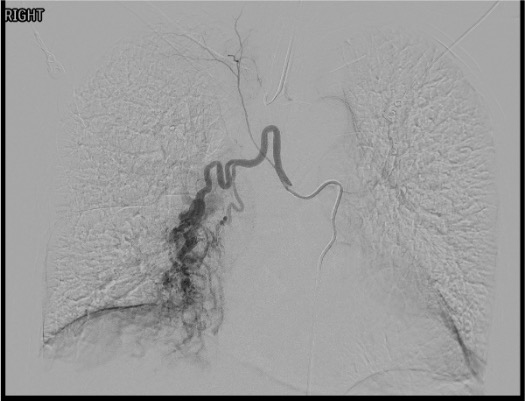
Selective Bronchial Artery Catheterization
Angiographic Assessment
Embolization
Search for Non-Bronchial Systemic Supply
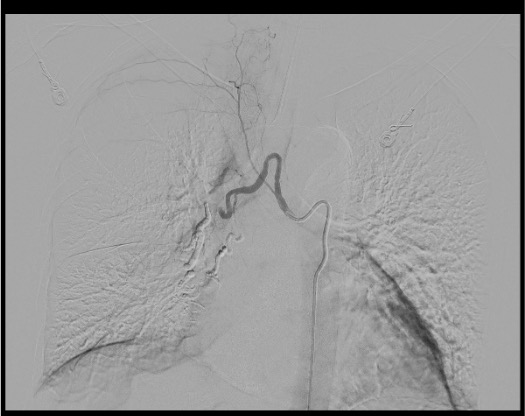
Completion Angiography
Community Cards
Key Landmarks
T5–T6 Aortic Level
- Primary origin of ~70% of bronchial arteries
- Center your aortogram here
- Corresponds roughly to the carina / left mainstem bronchus on fluoroscopy
- If no bronchial arteries found at this level, extend search above and below
ICBT Identification
- Right intercostobronchial trunk is the most common right-sided bronchial artery configuration
- Arises from the right posterolateral aorta
- Gives off the right bronchial artery + right intercostal artery
- The intercostal branch may supply the anterior spinal artery — always check
Spinal Artery Hairpin Sign
- Small branch coursing medially toward the spinal canal
- Makes a sharp “hairpin” turn as it joins the anterior spinal artery
- If seen: STOP — do NOT embolize that vessel from this position
- Advance microcatheter distal to spinal artery origin or abandon vessel
Troubleshooting
No Abnormal Bronchial Arteries Identified at T5–T6
Perform complete thoracic aortogram to identify ectopic bronchial arteries arising outside the T5–T6 level. Search for non-bronchial systemic collateral supply: intercostal arteries, internal mammary artery, subclavian branches, thyrocervical trunk, inferior phrenic arteries. Up to 30% of bronchial arteries have ectopic origins. If no arterial source found, consider pulmonary angiogram to evaluate for pulmonary artery bleeding source.
Anterior Spinal Artery Seen on Selective Angiogram
ABORT embolization of that artery from current catheter position. Options: advance microcatheter beyond spinal artery origin to achieve distal purchase and embolize from there (only if safe distance confirmed), or abandon that vessel entirely. Never embolize proximal to a visible spinal artery origin. Document finding. Consider provocative testing with intra-arterial lidocaine if occult spinal supply is suspected in other vessels.
Recurrent Bleeding Days to Months After Initial Embolization
Recurrence rate is 10–30% at 1 year. Most commonly due to missed non-bronchial systemic collateral supply at initial procedure. Repeat CTA and re-angiogram. Systematically interrogate ALL potential systemic supply: intercostals, IMA, subclavian branches, inferior phrenic. Also evaluate for recanalization of previously embolized vessels. Pulmonary artery source should be excluded if no systemic source identified.
Unable to Select Bronchial Artery Ostia
Bronchial artery anatomy is highly variable. Try multiple catheter shapes: Cobra C2, SOS Omni, Mikaelson, Simmons. Consider reverse-curve catheter (Simmons) for acute angulation origins. Use a microcatheter/microwire coaxial system for subselective access. If ostium cannot be engaged, perform aortogram to redefine anatomy and attempt from different projection angle.
Complications
Common / Expected
- Chest pain / pleuritic pain — most common; typically transient 2–7 days post-embolization; treated with analgesics; may require IV corticosteroids
- Dysphagia — esophageal branch embolization; usually transient; self-resolves in days
- Low-grade fever — post-embolization syndrome; supportive care
- Groin hematoma — femoral access site complication; standard management
Serious Complications
- Spinal cord ischemia / paralysis (<5%) — most feared complication; due to anterior spinal artery embolization; can be devastating and irreversible; bilateral lower extremity weakness post-procedure = emergency imaging and neurology
- Recurrence (10–30% at 1 year) — missed non-bronchial systemic supply, recanalization, disease progression
- Bronchial necrosis (rare) — non-target embolization of bronchial wall supply
- Pulmonary infarction (rare) — in setting of compromised pulmonary arterial supply
- Aortic dissection (rare) — catheter-related injury
Pearls & Pitfalls
References & Resources
Standards of Practice
- CIRSE SoP: Bronchial Artery Embolization → CIRSE Standards of Practice Committee
Primary References
- Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics. 2002;22(6):1395–1409.
- Swanson KL, Johnson CM, Prakash UB, McKusick MA, Andrews JC, Stanson AW. Bronchial artery embolization: experience with 54 patients. Chest. 2002;121(3):789–795.
- O’Dell MC, Gill AE, Hawkins CM. Bronchial artery embolization for the treatment of acute hemoptysis. Tech Vasc Interventional Rad. 2017;20:263–265.
- Chun JY, Morgan R, Belli AM. Radiological management of hemoptysis: a comprehensive review of diagnostic imaging and bronchial arterial embolization. Cardiovasc Interv Radiol. 2010;33:240–250.
- Lopez JK, Lee HY. Bronchial artery embolization for treatment of life-threatening hemoptysis. Semin Interv Radiol. 2006;23:223–229.