Indications / Contraindications
Indications
- Inability to achieve adequate peripheral venous access
- Medications unsafe via peripheral IV: TPN, vasopressors, chemotherapy, hypertonic solutions
- Frequent blood draws; central venous pressure monitoring
- Hemodialysis (acute); plasmapheresis
- Rapid volume resuscitation (large-bore access)
Contraindications
- Absolute: Combative/uncooperative patient; no safe access site
- Relative: Coagulopathy (SIR: INR ≤2.0, platelets ≥50K); active sepsis at proposed access site; prior radiation therapy traversing access site; suspected vein occlusion (confirm patency with US pre-procedure)
- Anticoagulation: Aspirin and Plavix do NOT need to be held. LMWH: hold 1 dose if feasible.
- Note: Clinical urgency frequently overrides ability to correct coagulopathy.
Pre-Procedure Checklist
Relevant Anatomy
Site-Specific Anatomy
- See Section 9 (Site Selection) for detailed site-by-site guide.
- IJ vein: Anterior-lateral to carotid artery; compressible on US; distends with Valsalva; right IJ provides direct path to SVC and right atrium
- Subclavian vein: Superficial to subclavian artery; distends with Valsalva; compressed under clavicle medially
- Femoral vein: Medial to femoral artery in femoral triangle; compressible; thrombosis risk ~20%
Target Tip Position
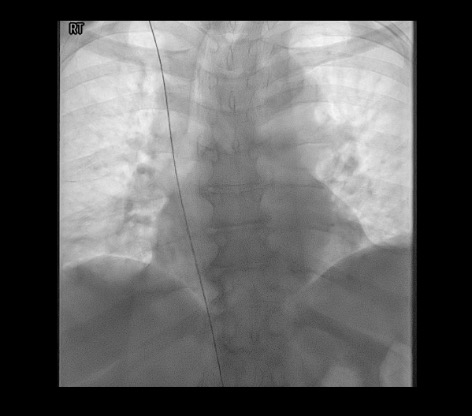
- IJ / Subclavian catheters: SVC–right atrial junction or upper right atrium (confirmed fluoroscopically)
- Femoral catheters: Tip at IVC–right atrial border
- Tip position must be confirmed fluoroscopically before line use
- Malposition into ipsilateral IJ, azygos vein, or contralateral brachiocephalic should prompt repositioning over wire
Technique
Default RadCall approach · share your own below
Supplies
Steps
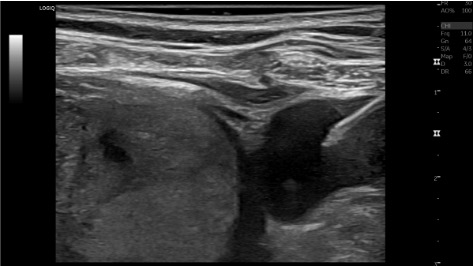
US survey
Positioning
Sterile prep + local anesthesia
Single-wall venipuncture
Microwire placement
Skin incision + blunt dissection
Exchange to 0.035" system
Catheter placement
Confirm + secure
Troubleshooting
Wire deflects superiorly (into IJ / not heading to SVC)
Likely cause: Needle tip not in SVC; wire following extravascular or wrong track; needle angled too superiorly.
Next step: Withdraw needle and wire as a unit. Reattempt with needle directed more caudally. Advance wire under fluoroscopy to confirm trajectory toward SVC before exchanging sheath.
Wire kinks on exit through skin
Likely cause: Skin incision too small; subcutaneous tract not adequately blunt dissected.
Next step: Replace with new wire. Ensure skin incision is adequate and bluntly dissect the tract with mosquito hemostat before re-exchanging.
Cannot compress vein / suspected thrombosis
Likely cause: Acute or chronic DVT at target site.
Next step: Perform full US survey; confirm with power Doppler. Do NOT puncture thrombosed vein. Switch to alternative site.
Inadvertent carotid / arterial puncture
Likely cause: Medial needle trajectory; excessive pulsatile flow on aspiration; bright red blood.
Next step: Remove needle; apply gentle pressure × 5–10 min. Abandon this access level; reassess and attempt IJ at different level or opposite side. If large sheath already placed in carotid — do NOT remove at bedside (risk of massive hematoma) — vascular surgery emergency.
No blood return
Likely cause: Needle not deep enough; posterior wall puncture; needle outside lumen.
Next step: Advance needle slightly under US; rotate bevel; try repuncture. Needle may have passed through posterior wall — withdraw slowly under US while aspirating.
Catheter kinking at skin
Likely cause: Skin incision too small; subcutaneous tract underdissected.
Next step: Pull back catheter; enlarge incision with hemostat; re-advance catheter.
Air embolism (sudden hemodynamic collapse, "mill-wheel" murmur)
Likely cause: Air entrainment during sheath exchange or catheter placement; hub left open.
Next step: Immediately left lateral decubitus + Trendelenburg; 100% O2; aspirate through catheter; hyperbaric O2 if available.
Complications
Procedural
- Arterial puncture (1–3%): Remove needle, firm pressure ×10 min. Do not dilate or place catheter in artery. If large sheath placed in carotid — do NOT remove at bedside — vascular surgery emergency.
- Pneumothorax (1–3%, IJ/subclavian): Uncommon with US guidance. Small/stable → supplemental O2 ± serial CXR. Large/symptomatic → small-bore chest tube.
- Hematoma (1–3%): Compression; usually self-limited.
- Air embolism (<1%): See troubleshooting above.
Delayed
- CLABSI (1–3%): Remove non-tunneled line; blood cultures; IV antibiotics; place new line if still needed.
- Venous thrombosis: IJ/subclavian ~4%; femoral ~20%. Anticoagulation; remove catheter when no longer needed.
- Catheter malposition: Detected on CXR; requires repositioning over wire under fluoroscopy.
- Overall major complication rate with image guidance: ~3%; technical success >99% with US guidance.
Post-Procedure Care
Confirmation + Securing
- Fluoroscopic confirmation of tip at SVC-RA junction required before use
- Line secured with 2-0 nonabsorbable suture ×2 sites; Biopatch at skin entry
- All lumens flushed with heparinized saline; volume per lumen marked on catheter
Ongoing Line Care
- Daily assessment of line necessity — remove as soon as no longer needed (reduces CLABSI risk)
- Dressing change per institutional protocol (usually q7d with chlorhexidine-impregnated dressing)
- Suspected CLABSI: Draw blood cultures from line AND peripheral; consider catheter removal
Critical Pearls
Site Selection
Site-by-site anatomy, technique, and tradeoffs
| Site | Status | Anatomy & Technique | Advantages | Avoid When |
|---|---|---|---|---|
| Right IJ | Preferred | Anterior-lateral to carotid; larger caliber than left IJ; direct straight path to SVC and RA. US probe parallel/cephalad to clavicle; target lateral wall of IJ; puncture low (near clavicle); keep carotid visible on US at all times. | Least complication risk; easiest tunneling if conversion to tunneled dialysis catheter needed. | Right neck lymphadenopathy, prior radiation, or ipsilateral AV fistula planned. |
| Left IJ | Acceptable | Two ~90° turns at IJ-brachiocephalic junction and brachiocephalic-SVC junction. Use stiff hydrophilic wire to navigate turns; advance wire under fluoroscopy. | Acceptable alternative when right IJ unavailable. | Slightly higher catheter kink and malposition rate vs. right IJ. Avoid if right IJ is accessible. |
| External Jugular (EJ) | Acceptable | Visible and palpable lateral neck; US identifies it superficial to the SCM. Advance wire carefully — acute angle at EJ–subclavian junction; hydrophilic wire or stiff wire may be needed. Direct visualization often possible without US. | No arterial puncture risk. Viable when both IJ sites are occluded or unavailable. | Tortuous anatomy common; higher malposition rate. Reserve for cases where IJ is inaccessible. |
| Subclavian | Caution | Access via lateral half of clavicle (avoids "pinch-off" at medial clavicle-rib compression). Transducer perpendicular to clavicle — simultaneously visualize subclavian vein, artery, and pleura. Left subclavian preferred over right (less acute angle into SVC). | Acceptable when IJ sites unavailable. Lower infection rate than femoral. | Any patient who may ever need hemodialysis (AV fistula/graft outflow). Associated with higher rates of subclavian stenosis, thrombosis, and irreversible compromise of upper extremity AV access. Pneumothorax risk 1–3%. |
| Femoral | Last Resort | Femoral vein is medial to femoral artery; access ideally over femoral head. Needle at 45° aiming cephalad; advance 5 mm medial to femoral arterial pulse. Tip position: IVC–right atrial border (not SVC-RA junction). | No pneumothorax risk; useful in coagulopathic patients where compression is feasible; accessible during CPR. | Ambulatory patients; immunocompromised; patients who will be mobilized. Thrombosis rate ~20%; highest infection risk of all sites. |
References & Resources
Key Guidelines
- SIR Standards of Practice for Venous Access
- ACR-SIR-SPR Practice Parameter for Central Venous Access
- SCCM/IDSA CLABSI Prevention 2022
Primary References
- McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348(12):1123-1133.
- Sznajder JI et al. Central vein catheterization: failure and complication rates by three percutaneous approaches. Arch Intern Med. 1986;146(2):259-261.
- Troianos CA et al. Guidelines for performing ultrasound guided vascular cannulation. J Am Soc Echocardiogr. 2011;24(12):1291-1318.
- Brass P et al. Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev. 2015;(1):CD011447.