Splenic Artery Embolization — Trauma, Aneurysm, and Hypersplenism
Splenic artery embolization (SAE) is a spleen-preserving alternative to splenectomy for blunt splenic trauma, splenic artery aneurysm, and symptomatic hypersplenism. Technique selection between proximal (main trunk) and distal (selective parenchymal) approaches depends on indication, injury grade, and hemodynamic status — each with distinct hemodynamic and infarction profiles.
Key points
Primary trauma indication: hemodynamically stable blunt splenic injury with AAST grade III–V, CT evidence of contrast extravasation, pseudoaneurysm, or AV fistula. Non-operative management with SAE has splenic salvage rates >85% and lower morbidity than splenectomy.
Proximal vs distal embolization: proximal (main splenic artery distal to dorsal pancreatic and pancreatica magna branches) reduces splenic perfusion pressure and preserves collateral flow — used for diffuse injuries or multiple bleeding points. Distal (superselective) targets specific pseudoaneurysm or extravasation — used for focal injuries.
Aneurysm indications: any splenic artery pseudoaneurysm; true aneurysm >2 cm, enlarging, symptomatic, in women of childbearing age, or pre-liver transplant.
Hypersplenism: partial splenic embolization (PSE) with particulate embolics (Gelfoam, PVA) to infarct 50–70% of splenic parenchyma, reducing splenic sequestration while preserving immune function.
Embolic selection: coils and vascular plugs for proximal and aneurysm embolization; microcoils, Gelfoam slurry, or particles for distal/selective; covered stents for select wide-neck aneurysms with preservation of splenic flow.
AAST grade III–V with contrast blush, pseudoaneurysm, AV fistula, or moderate-to-large hemoperitoneum — see abdominal solid organ trauma imaging
Splenic artery pseudoaneurysm (any size)
Traumatic, post-pancreatitis, iatrogenic — high rupture risk; treat promptly
Splenic artery true aneurysm
>2 cm, enlarging, symptomatic, in pregnancy or women of childbearing age, pre-transplant
Symptomatic hypersplenism
Refractory thrombocytopenia or anemia in cirrhosis, hematologic disease; partial splenic embolization
Pre-operative devascularization
Reduce blood loss prior to laparoscopic or difficult open splenectomy
Splenic vein thrombosis with gastric varices (segmental portal HTN)
SAE reduces splenic inflow and pressures on gastric varices as adjunct therapy
Type
Contraindication
Absolute
Hemodynamic instability despite resuscitation (go to OR) · Uncorrectable coagulopathy when rapid control is needed
Relative
Severe contrast allergy · Renal impairment · Prior celiac or splenic artery occlusion limiting access
AAST Splenic Injury Grading (2018 Revision)
Grade
Imaging / Injury
I
Subcapsular hematoma <10% surface area; laceration <1 cm depth
II
Subcapsular hematoma 10–50%; intraparenchymal hematoma <5 cm; laceration 1–3 cm
III
Subcapsular hematoma >50% or expanding; intraparenchymal hematoma ≥5 cm; laceration >3 cm
IV (2018 revision: vascular injury)
Any injury with vascular injury or active bleeding contained within splenic capsule; laceration involving segmental or hilar vessels >25% devascularization
V
Shattered spleen; hilar vascular injury devascularizing the spleen; any active bleeding extending beyond the spleen into the peritoneum
The 2018 revision incorporates vascular injury (contrast extravasation, pseudoaneurysm, AV fistula) into the CT-based grade (upgrading to IV), which aligns angiography-eligible patients with intervention.
Splenic Arterial Anatomy
Splenic artery arises from the celiac trunk; tortuous course along the superior pancreas.
Key branches: dorsal pancreatic artery (proximal), pancreatica magna (mid), short gastric arteries (distal), left gastroepiploic, and terminal splenic branches at the hilum.
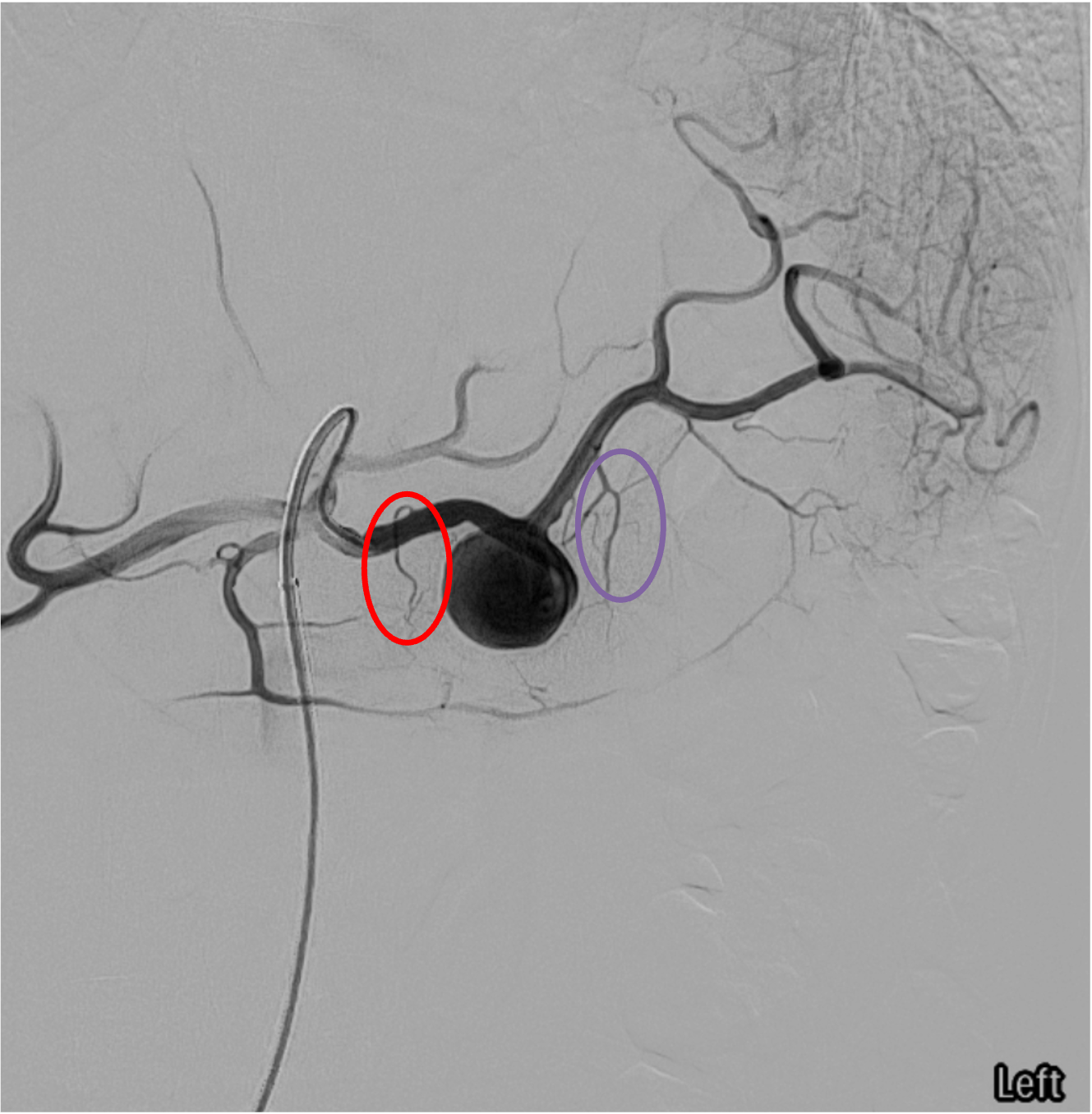
For proximal embolization: deploy distal to the dorsal pancreatic and pancreatica magna origins but proximal to the hilum — preserves pancreatic blood supply and allows collateral flow from short gastrics and gastroepiploics to maintain splenic perfusion at reduced pressure.
Splenic artery anatomy — key branching landmarks for proximal embolization targeting.Splenic angiogram — dorsal pancreatic artery (red) and pancreatica magna (purple); proximal embolization target is distal to these branches.
Procedure Overview
The following is a high-level summary. Full coil and plug sizing matrices, Gelfoam slurry preparation, and damage-control-angiography timing are available in RadCall Pro.
Access and Diagnostic Angiography
Access: right common femoral artery; 5–6 Fr sheath. Radial access feasible in select patients.
Celiac trunk angiogram with cobra, Simmons, or Sos catheter to confirm anatomy and identify splenic artery, branching, and any extravasation or pseudoaneurysm.
Selective splenic angiogram: advance catheter into splenic artery; identify target (extravasation, pseudoaneurysm, AV fistula, or perfusion distribution for PSE).
Proximal vs Distal Technique Selection
Technique
Best application
Advantages
Trade-offs
Proximal (main splenic artery distal to pancreatica magna)
Occludes focal lesion plus reduces overall perfusion pressure
Higher total infarction rate
Embolic Agent Selection
Agent
Application
Amplatzer vascular plug (AVP II/IV)
Proximal main splenic artery occlusion; single device; fast deployment
Lobo Occluder (Okami Medical)
Proximal main splenic artery; sizes 3–9 mm (LOBO-3/5/7/9); delivered via SENDERO microcatheter; minimal CT artifact, MR Conditional; no spinnaker effect
Pushable fibered coils
Proximal trunk; aneurysm sac packing; large delivery tip
Post-pancreatitis pseudoaneurysm: higher re-bleed rate; close follow-up imaging.
Splenic artery aneurysm — saccular dilation of the splenic artery trunk amenable to coil sandwich or covered stent exclusion.
Partial Splenic Embolization (Hypersplenism)
Superselective distal branch embolization with Gelfoam or particles to infarct a target 50–70% of parenchyma.
Preserves sufficient splenic immune function while reducing sequestration of platelets and red cells.
Staged if ≥70% infarction would be required — higher abscess and post-embolization syndrome.
Immunization: consider pneumococcal, meningococcal, and Haemophilus influenzae type b vaccines for patients undergoing functional splenectomy (large partial embolization, extensive infarction). Not required for focal distal embolization with preserved parenchyma.
Analgesics, antipyretics; usually 3–7 days; differentiate from abscess with imaging/cultures if persistent
Splenic infarction >50%
Variable (higher with distal and combined)
Expectant; watch for abscess; most tolerated well
Splenic abscess
1–3%
Percutaneous drainage and antibiotics; rare splenectomy
Pancreatitis
1–3%
Usually mild; proximal embolization distal to pancreatica magna prevents
Rebleeding requiring splenectomy
5–10% in trauma
Hemodynamic deterioration → OR
Non-target embolization (gastric, pancreatic)
<2%
Selective catheter placement and careful injection prevent
Coil/plug migration
<1%
Proper sizing; snare retrieval if problematic
OPSI (overwhelming post-splenectomy infection)
Low with preserved parenchyma
Vaccinate if >70% infarction
Post-Procedure Care
Admission: ICU or monitored bed for trauma; follow serial hemoglobin and vital signs.
Imaging follow-up: contrast CT at 24–72h for trauma to assess infarct extent and exclude complications; additional CT if clinical deterioration.
Analgesia and antiemetics for post-embolization syndrome.
Discharge: trauma — typically 3–7 days; aneurysm — 1–2 days.
Outpatient follow-up: CT at 1–3 months for aneurysm exclusion; platelet/CBC trending for hypersplenism.
Evidence Summary
Stassen NA et al (2012, EAST guidelines, J Trauma Acute Care Surg): non-operative management with SAE recommended for hemodynamically stable high-grade injuries with vascular findings; improves splenic salvage.
Schnüriger B et al (2011, J Trauma) and systematic reviews: proximal SAE has similar failure rate to distal SAE with fewer complications; selection depends on injury pattern.
Kozar RA et al (2018, J Trauma Acute Care Surg): AAST 2018 OIS revision incorporates vascular injury into CT-based grading, improving alignment with intervention.
Akinci D et al (2008): pseudoaneurysm and splenic artery true aneurysm treatment — coils and covered stents yield durable exclusion with low morbidity.
Madoff DC et al (2005, RadioGraphics): splenic artery embolization techniques and outcomes review — foundational reference.
References
Stassen NA, Bhullar I, Cheng JD, et al. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S294–S300.
Kozar RA, Crandall M, Shanmuganathan K, et al. Organ injury scaling 2018 update: spleen, liver, and kidney. J Trauma Acute Care Surg. 2018;85(6):1119–1122.
Schnüriger B, Inaba K, Konstantinidis A, Lustenberger T, Chan LS, Demetriades D. Outcomes of proximal versus distal splenic artery embolization after trauma: a systematic review and meta-analysis. J Trauma. 2011;70(1):252–260.
Madoff DC, Denys A, Wallace MJ, et al. Splenic arterial interventions: anatomy, indications, technical considerations, and potential complications. RadioGraphics. 2005;25(Suppl 1):S191–S211.
Abdel-Aal AK, Hamed MF, Biosca RF, Saddekni S. Transcatheter embolization of splenic artery aneurysms and pseudoaneurysms. AJR. 2014;202(4):W310–W316.
Al-Habbal Y, Christophi C, Muralidharan V. Aneurysms of the splenic artery — a review. Surgeon. 2010;8(4):223–231.
Full technique in RadCall Pro
Coil and plug sizing matrices, Gelfoam slurry preparation, AAST-to-technique decision algorithm, and damage-control-angiography timing available in RadCall Pro.