Percutaneous Renal Tumor Ablation — Cryo, RFA, and Microwave
Percutaneous ablation is an established, guideline-supported treatment for localized renal tumors with the strongest evidence for cT1a masses ≤3 cm, where oncologic outcomes are comparable to partial nephrectomy in terms of metastasis-free and cancer-specific survival — with lower morbidity and superior renal function preservation. Cryoablation, radiofrequency ablation (RFA), and microwave ablation (MWA) each have distinct profiles with modality selection driven by tumor size, location, and proximity to critical structures.
Key points
Guideline support: NCCN (v2.2026) lists percutaneous ablation as category 2A for cT1a and 2B for select cT1b. AUA 2021 recommends thermal ablation as a reasonable alternative for tumors <3 cm; percutaneous approach preferred over laparoscopic. SIR affirms similar cancer-specific survival with fewer complications vs. partial nephrectomy.
Oncologic equivalence for T1a: Danish nationwide registry (n=1,862): no significant difference in progression risk vs. surgical resection (HR 1.46; p=0.40); distant metastasis actually more frequent after nephrectomy (4.38% vs. 1.67%; p=0.02).
Best evidence size threshold: ≤3 cm. Optimal TRIFECTA cutoff is 3.2 cm. Exophytic location predicts success regardless of size. For 3–4 cm tumors, cryoablation outperforms heat-based modalities (DeGIR registry, n=1,102).
MWA vs. RFA: MWA has fewer local recurrences (OR 0.31; p=0.0008), fewer complications vs. RFA (OR 0.60) and cryoablation (OR 0.49), and superior TRIFECTA achievement (84.2% vs. 72.2%).
Long-term cryoablation: 15-year disease-specific survival 99%, local PFS 95% in a 307-patient series. 10-year prospective study: DSS 94% at 5 and 10 years; 10-year hemodialysis risk only 2.3%.
Renal function: eGFR decline 4.47 mL/min/1.73 m² after ablation vs. 13.09 after partial nephrectomy. Critical advantage for solitary kidney, CKD, or bilateral tumors.
Pre-procedure biopsy is standard — NCCN, AUA, and SIR all recommend biopsy prior to or at the time of ablation; ablated tissue cannot be re-evaluated.
Guideline Recommendations
Guideline
Recommendation
NCCN Kidney Cancer v2.2026
Percutaneous ablation (cryoablation, RFA, MWA) as a category 2A option for cT1a (≤4 cm) tumors; category 2B for select cT1b (4.1–7 cm) not eligible for surgery. Biopsy recommended prior to or at the time of ablation. May require retreatment to achieve equivalent local oncologic outcomes to surgery.[1]
AUA 2021
Thermal ablation is a reasonable alternative for tumors <3 cm. Percutaneous approach preferred over laparoscopic — shorter procedure time, quicker recovery, lower narcotic requirements.[2]
SIR Position Statement
Ablation offers similar cancer-specific survival with fewer complications compared to partial nephrectomy for T1a RCC. Lower perioperative complication rate: 12.5% vs. 17.0% for PN. Advocates inclusion in multidisciplinary treatment discussions.[5]
Indications and Contraindications
Indication
Notes
cT1a renal cell carcinoma (≤4 cm)
Primary indication; strongest evidence for ≤3 cm; outcomes comparable to partial nephrectomy
Solitary kidney or CKD
Nephron-sparing priority; eGFR decline 4.47 vs. 13.09 mL/min/1.73 m² after ablation vs. PN[24]
Hereditary syndromes
VHL, Birt-Hogg-Dubé, HLRCC — multiple tumors expected; serial ablations preserve function
Bilateral or multifocal tumors
Staged ablation preferred over bilateral surgery
Unfit for or declining surgery
Frailty, cardiopulmonary comorbidity; ablation under moderate sedation feasible
Select cT1b (4.1–7 cm)
Expanding indication; cryoablation achieves 95% primary efficacy; ice-ball margin ≥8 mm critical for local control[20]
Type
Contraindication
Absolute
Uncorrectable coagulopathy · Active untreated infection · Metastatic disease with short life expectancy
Relative
Tumor >4 cm (higher residual risk) · Central/hilar location near collecting system (requires pyeloperfusion) · Adjacent bowel <1 cm (requires hydrodissection) · Upper-pole proximity to pleura (pneumothorax risk)
Ablation vs. Partial Nephrectomy: Oncologic Outcomes
Study
n
Key Finding
Danish nationwide registry (Radiology 2026)[4]
1,862
No significant difference in progression risk vs. surgical resection for T1a RCC (HR 1.46; 95% CI 0.60–3.56; p=0.40). Local recurrence slightly higher after ablation (2.41% vs. 1.20%; p=0.007) but treatable. Distant metastasis more frequent after nephrectomy (4.38% vs. 1.67%; p=0.02). Median hospital stay 0 days for ablation vs. 2 days.
Propensity-matched analysis (Urology 2025)[6]
12,546
Comparable 10-year survival: PN 89.4%, cryoablation 89.2%, heat-based ablation 87.8% (p>0.05). Higher reintervention rates at 10 years for ablation (cryoablation 13.0%, heat-based 9.6% vs. PN 1.3%).
Mayo Clinic series (Eur Urol 2019)[7]
1,798
No significant differences in local recurrence, metastases, or RCC death for cT1a. 5-year CSS: PN 99%, RFA 96%, cryoablation 100%. cT1b: differences in RCC-related death could not be excluded.
Meta-analysis of comparative trials (Front Oncol 2023)[8]
2,107
Significantly less eGFR decline after ablation (WMD −9.84 mL/min/1.73 m²; p<0.05). Ablation had lower procedural morbidity but higher reintervention rates.
Modality Comparison
Local Control by Modality — Lancet Oncology Meta-Analysis (2025)[9]
133 studies, n=8,910 patients — most comprehensive comparison of all ablative modalities:
Modality
1-yr Local Control
2-yr Local Control
5-yr Local Control
Grade 3–4 AEs
SBRT
99% (97–100)
97% (95–99)
95% (89–98)
2%
RFA
96% (94–98)
95% (92–98)
92% (88–96)
2%
MWA
97% (95–99)
95% (92–98)
86% (75–94)
1%
Cryoablation
95% (93–96)
94% (91–96)
90% (87–93)
3%
Head-to-Head Modality Data
Comparison
Key Findings
MWA vs. RFA[10][11]
Meta-analysis (10 studies, n=2,258): MWA had fewer local recurrences than RFA/cryoablation (OR 0.31; p=0.0008) and fewer overall complications than RFA (OR 0.60; p=0.04) and cryoablation (OR 0.49; p=0.01). Single-center series (n=531): MWA superior TRIFECTA achievement (84.2% vs. 72.2%; p=0.001) and shorter operative time.
MWA vs. Cryoablation[12][13]
12-year single-center study (n=279): no significant differences in local recurrence, cancer-free survival, or overall survival after propensity matching. MWA had significantly shorter ablation time (WMD −24.6 min).
Cryo advantage for 3–4 cm tumors[14]
DeGIR registry (n=1,102): heat-based ablation had lower technical success (89.8% vs. 96.1%; p=0.005) and higher complication rates (11.1% vs. 3.9%; p=0.002) for 3–4 cm lesions. Cryoablation showed no size-dependent differences in this range.
Cryo advantage for central/hilar tumors[15]
Slower ice-ball formation allows real-time monitoring and reduces risk of collecting system injury. Preferred modality when collecting system is <4 mm from tumor margin.
Feature
Cryoablation
RFA
MWA
Mechanism
Ice-ball (Joule–Thomson); freeze–thaw cycles
Resistive heating via alternating current
Dielectric heating via EM field
Visible ablation zone
Yes — ice-ball visible on CT/MRI/US
No direct zone; gas/cavitation artifact
Limited; gas artifact
Heat-sink effect
Minimal
Significant near large vessels
Less than RFA
Ablation time
2 × 10 min freeze with 8 min thaw
10–20 min per cycle
2–10 min
Best application
Central, complex, larger tumors; 3–4 cm range
Small peripheral tumors; mature evidence base
Peripheral tumors; near large vessels; lowest complication rate
Grade 3–4 AEs (Lancet Onc)[9]
3%
2%
1%
Long-Term Cryoablation Outcomes
Cryoablation has the most mature long-term data among ablation modalities:
Morkos et al. (Radiology 2020) — 10-year prospective[17]
134 pts; 10-year prospective
DSS 94% at 5 and 10 years — equivalent to matched PN and RN cohorts from NCDB. 10-year risk of hemodialysis: 2.3%.
Breen et al. (Radiology 2018) — biopsy-proven RCC[18]
220 pts; biopsy-proven
5-year local recurrence-free survival 93.9%; metastasis-free survival 94.4%; major complication rate 4.9%.
T1b Tumors (4.1–7 cm): Expanding Indications
Ablation of T1b tumors remains more challenging, with higher local recurrence but acceptable outcomes in select patients:
Matched-pair analysis vs. robotic PN (AblatT1b, Eur Radiol 2023):[19] local recurrence higher after ablation (14.6% vs. 4%; p=0.02) but major complications higher after surgery (5.3% vs. 0%).
Cryoablation for T1b (JVIR 2025, n=80):[20] primary efficacy 95%, secondary efficacy 98.8%, 24-month local tumor progression-free survival 98.8%. Ice-ball margin ≥8 mm was critical — patients achieving this margin had 100% local control vs. 57% at 6 months for margins <8 mm.
Tertiary center series (CVIR 2026, n=51):[21] cryoablation ± embolization — 5-year local recurrence-free survival 87%, metastasis-free survival 96%, local recurrence rate 4%.
Tumor Size and Location: Predictors of Success
Optimal size threshold: ≤3 cm. A study of 432 patients identified 3.2 cm as the optimal cutoff for TRIFECTA achievement. Risk of failure increases for tumors >4 cm (OR 1.49).[22]
Exophytic location is a strong independent predictor of complete necrosis regardless of size. All exophytic tumors achieved complete necrosis in one series.[23]
Central/hilar tumors carry higher risk of collecting system injury with heat-based modalities; cryoablation with pyeloperfusion preferred. Both small size and exophytic location independently predict success.[15][23]
Renal Function Preservation
Ablation consistently demonstrates superior renal function preservation compared to surgery — particularly important for solitary kidneys, baseline CKD, and bilateral tumors:[8][24][25]
Treatment
eGFR Decline
Percutaneous ablation
−4.47 mL/min/1.73 m²
Microwave ablation (large MWA series, n=708)
−5.2% at 6 months
Partial nephrectomy
−13.09 mL/min/1.73 m² / −4.7% at 6 months
Radical nephrectomy
−32.9% at 6 months
Pre-Procedure Imaging and RENAL Score
Multiphase CT or MRI characterizes enhancement, size, laterality, polar location, exophytic fraction, and proximity to the collecting system. The RENAL nephrometry score stratifies tumor complexity:
Entirely above/below = 1; crosses polar line = 2; >50% across or between = 3
Low (4–6): favorable for any modality; outpatient
Intermediate (7–9): cryoablation often favored; may need pyeloperfusion
High (10–12): complex; cryoablation with pyeloperfusion; multidisciplinary review
Procedure Overview
The following is a high-level summary. Full probe placement templates, ice-ball size tables by probe type, pyeloperfusion flow rates, and sedation protocols are available in RadCall Pro.
Pre-Procedure
Pre-procedure imaging: CT/MRI with contrast; calculate RENAL score; plan probe trajectory and protective maneuvers.
Biopsy: core biopsy at the start of the ablation session (or prior) for histology — ablated tissue cannot be re-evaluated.
Anesthesia: moderate sedation for cryoablation (less procedural pain); general anesthesia for RFA or centrally located tumors.
Patient position: prone or oblique depending on tumor location; CT guidance is standard.
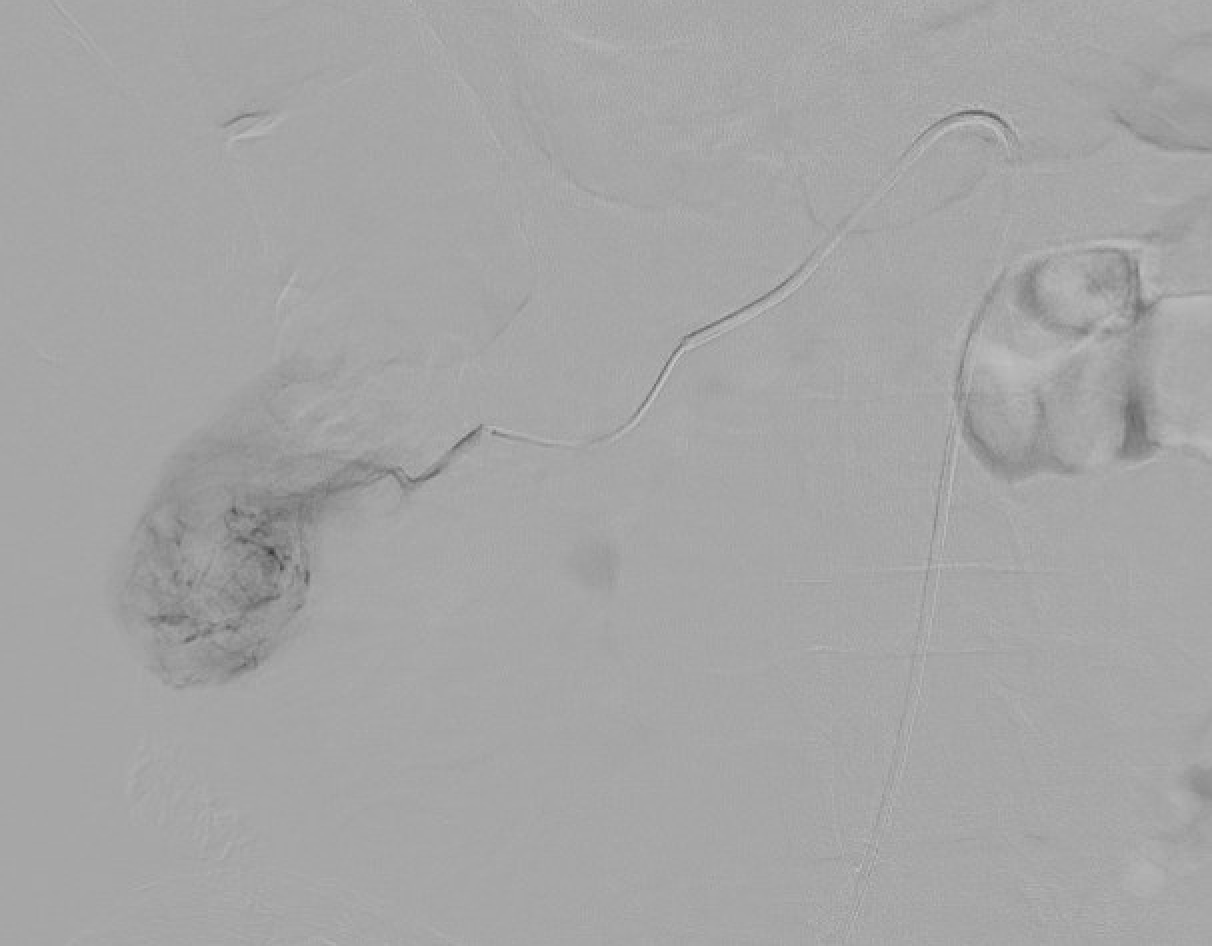
Pre-cryoablation renal mass with lipiodol tumor staining to define margins for probe placement.Pre-ablation angiogram demonstrating lipiodol tumor staining — selective injection used to mark tumor vascularity and guide probe targeting.
Protective Maneuvers
Hydrodissection: 5% dextrose (D5W — avoid saline for RFA; conductive) instilled to displace adjacent colon, duodenum, or psoas.
Pyeloperfusion: retrograde ureteral catheter placed pre-procedure; cooled D5W infused during ablation to protect urothelium for central tumors abutting the collecting system.
CO₂ or balloon displacement: rarely used to separate from diaphragm or adjacent structures.
Ablation
Probe placement under CT guidance: typically 1–6 probes for conformal ice-ball; avoid interlobar vessels and pelvicalyceal injury on trajectory.
Cryoablation cycle: 10 min freeze → 8 min passive thaw → 10 min freeze (two-cycle standard). Intermittent CT confirms ice-ball growth and margin. Target 5–10 mm ice-ball margin beyond tumor edge (cytotoxic −20°C to −40°C isotherm is several mm inside the visible edge).
RFA/MWA: energy delivered per manufacturer protocol; monitor temperature at margin; overlapping zones for larger tumors.
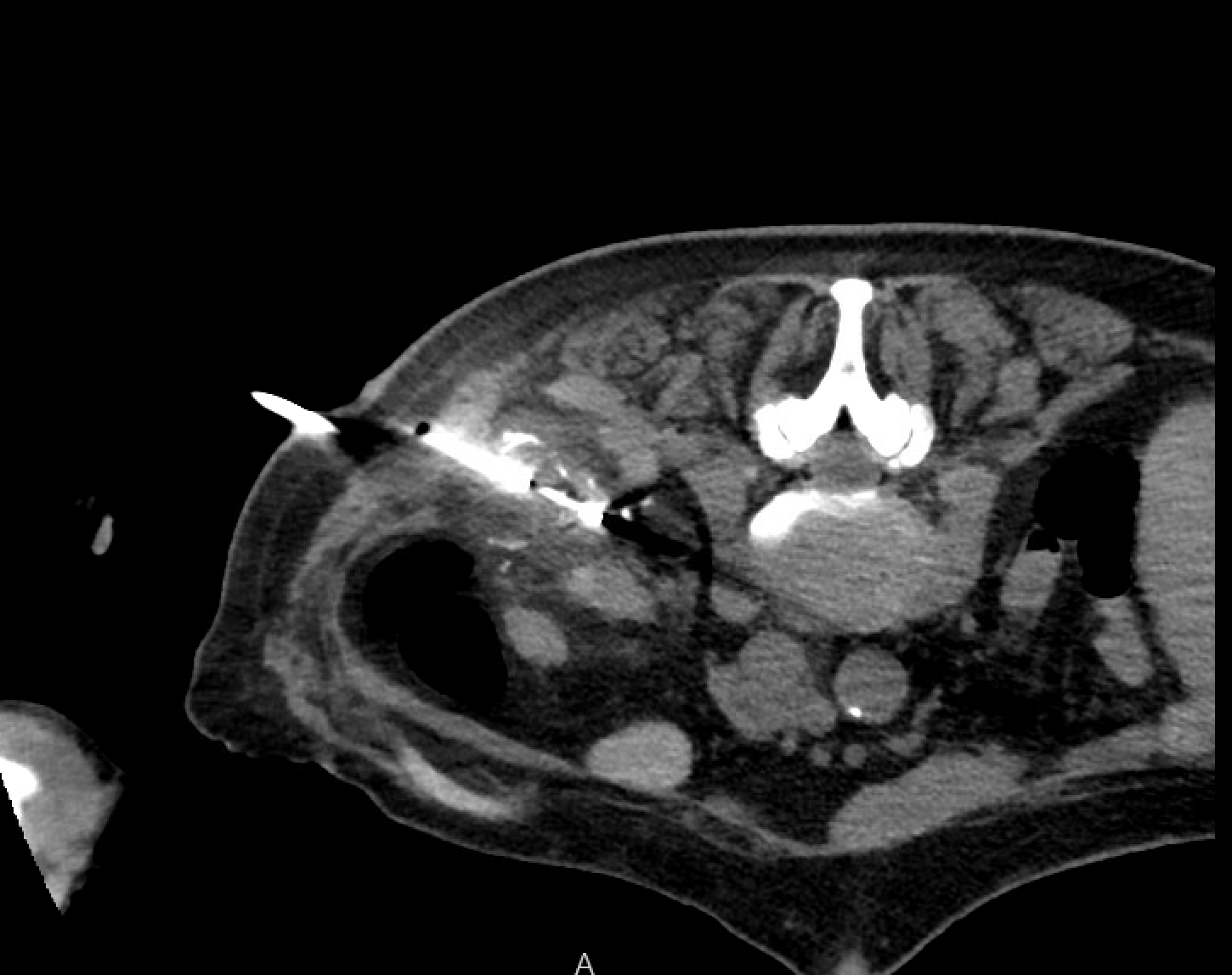
CT during cryoablation showing ice ball encompassing the renal mass — the hypodense ice ball should extend 5–10 mm beyond the tumor edge to achieve adequate lethal margin.
Immediate post-ablation CT: non-contrast and contrast-enhanced to confirm hypoenhancing ablation zone encompassing tumor plus margin; exclude active hemorrhage.
Post-Ablation Imaging Surveillance
Contrast-enhanced CT or MRI at 1, 3, 6, 12 months, then annually:
Finding
Expected
Concerning for Residual/Recurrent Disease
Ablation zone size
Initially larger than tumor (halo); gradual involution over 1–2 years
Re-growth on serial imaging
Enhancement
Non-enhancing (≤10–20 HU on CT)
Any nodular enhancement or >20 HU at margin
Rim enhancement
Thin smooth peripheral rim in first 3–6 months (reactive)
Thick, nodular, or progressive rim
Perinephric fat
Stranding, fluid collection acutely
Mass effect, soft-tissue nodule
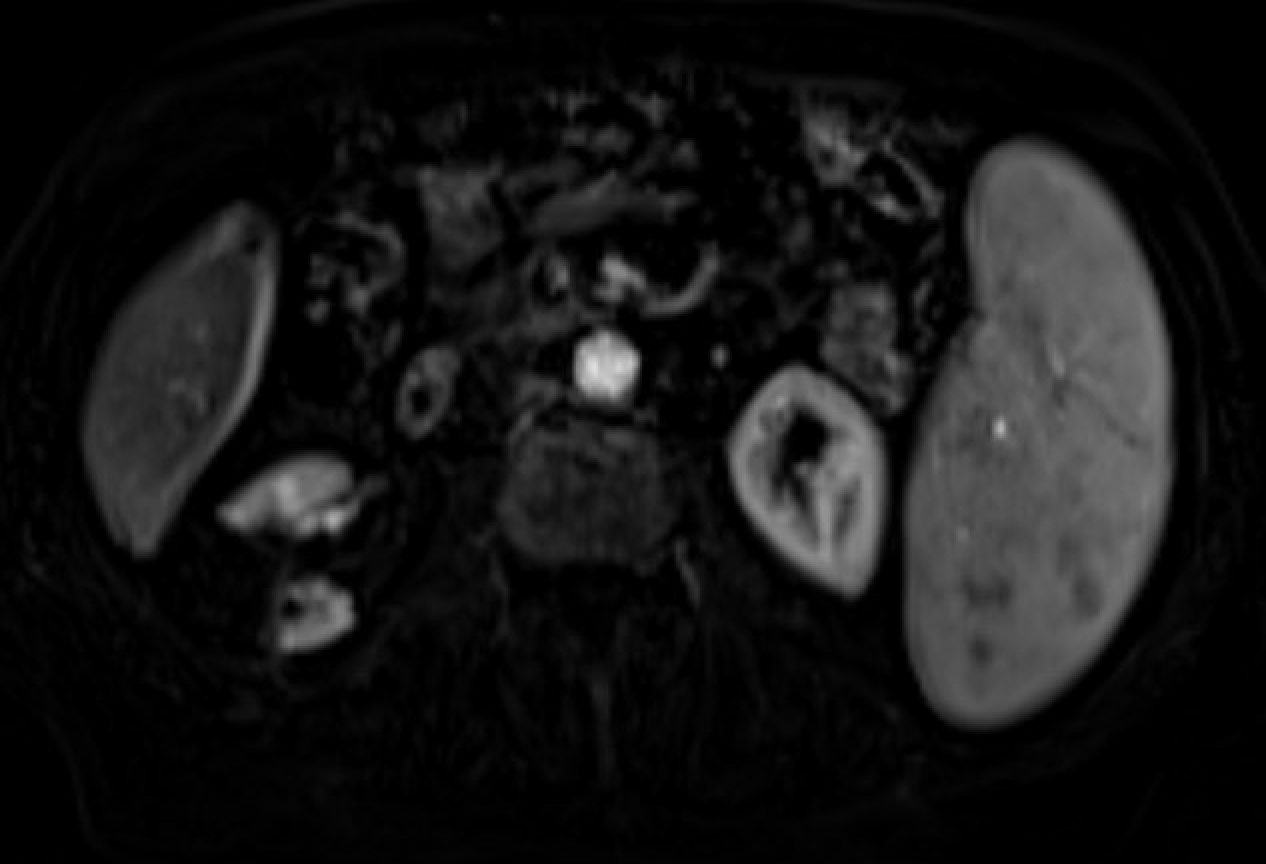
Follow-up MRI demonstrating no residual enhancement within the ablation zone after renal mass cryoablation — consistent with complete ablation and treatment success.
Complications
Overall complication rates are low — 8–14% overall, 2–5% major — and significantly lower than partial nephrectomy (SIR: 12.5% vs. 17.0%).[5][26]
Complication
Rate
Management
Perinephric hematoma
5–15% (most self-limited)
Observation; transfusion or embolization rarely required
Clinically significant hemorrhage
2–4%
Selective angioembolization
Urothelial injury / urine leak / urinoma
0–4%
Ureteral stenting; pyeloperfusion prevents
UTI
~2%
Antibiotics
Pneumothorax (upper-pole tumors)
1–5%
Observation or catheter drainage
Bowel injury
<1%
Hydrodissection prevents; surgical repair if occurs
Ureteral stricture
<1%
Central tumors; pyeloperfusion protective
Tract seeding
Very rare
Track ablation on probe withdrawal
Evidence Summary
Ahrenfeldt J et al (Radiology 2026) — Danish registry, n=1,862: no significant difference in progression risk between ablation and surgery for T1a RCC (HR 1.46; p=0.40); distant metastasis more frequent after nephrectomy (4.38% vs. 1.67%); hospital stay 0 days (ablation) vs. 2 days.[4]
Huang RS et al (Lancet Oncology 2025) — 133 studies, n=8,910: comprehensive modality comparison; SBRT highest 5-yr control (95%); RFA 92%; cryo 90%; MWA 86%; Grade 3–4 AEs lowest with MWA (1%).[9]
Stamper M et al (Urology 2025) — propensity-matched, n=12,546: comparable 10-year survival across PN, cryoablation, heat-based ablation (all ~87–89%; p>0.05); higher reintervention rates for ablation.[6]
Castellana R et al (Eur J Radiol 2023) — MWA vs. RFA/cryo meta-analysis, n=2,258: MWA fewest local recurrences (OR 0.31; p=0.0008), fewest complications.[10]
Bhagavatula SK et al (Radiology 2020) — cryo long-term, n=307: 15-yr DSS 99%, local PFS 95%; primary efficacy 96%, secondary 99%.[16]
Morkos J et al (Radiology 2020) — 10-yr prospective cryo, n=134: DSS 94% at 5 and 10 years; 10-yr hemodialysis risk 2.3%.[17]
Andrews JR et al (Eur Urol 2019) — Mayo Clinic, n=1,798: no significant differences in local recurrence, metastases, or RCC death for T1a; 5-yr CSS cryo 100%, RFA 96%, PN 99%.[7]
Schaarschmidt BM et al (Eur Radiol 2025) — DeGIR registry, n=1,102: heat-based ablation lower success (89.8% vs. 96.1%) and higher complications (11.1% vs. 3.9%) for 3–4 cm lesions; cryoablation size-independent.[14]
References
Kidney Cancer. National Comprehensive Cancer Network. Updated 2026-04-14. Version 2.2026.
Campbell SC, Clark PE, Chang SS, et al. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline: Part I. J Urol. 2021;206(2):199–208.
Roadman DF, Shapiro DD, Das A, et al. Percutaneous Microwave Ablation Preserves Renal Function With Similar Long Term Oncologic Outcomes Compared to Surgery for Clinical T1 RCC. Cancers. 2026;18(2):334.
Ahrenfeldt J, Jespersen J, Tonnesen P, et al. Ablation and Surgery Show Comparable Long-Term Outcomes for T1a Renal Cell Carcinoma: A Danish Nationwide Registry Study. Radiology. 2026;318(3):e251485.
Morris CS, Baerlocher MO, Dariushnia SR, et al. SIR Position Statement on the Role of Percutaneous Ablation in Renal Cell Carcinoma. J Vasc Interv Radiol. 2020;31(2):189–194.
Stamper M, Collins J, Arellano R, et al. Long-Term Outcomes of Partial Nephrectomy Versus Percutaneous Ablation for RCC: A Propensity-Matched Analysis. Urology. 2025. doi:10.1016/j.urology.2025.07.065.
Andrews JR, Atwell T, Schmit G, et al. Oncologic Outcomes Following Partial Nephrectomy and Percutaneous Ablation for cT1 Renal Masses. Eur Urol. 2019;76(2):244–251.
Wen Z, Wang L, Huang J, et al. Perioperative, Functional, and Oncologic Outcomes After Ablation or Partial Nephrectomy for Solitary Renal Tumors: Systematic Review and Meta-Analysis. Front Oncol. 2023;13:1202587.
Huang RS, Chow R, Benour A, et al. Comparative Efficacy and Safety of Ablative Therapies in Primary Localised Renal Cell Carcinoma. Lancet Oncol. 2025;26(3):387–398.
Castellana R, Natrella M, Fanelli G, et al. Efficacy and Safety of MWA Versus RFA and CA for Renal Tumors: Systematic Review and Meta-Analysis. Eur J Radiol. 2023;165:110943.
Jannello LMI, Orsi F, Luzzago S, et al. Microwave vs Radiofrequency Ablation for Small Renal Masses. BJU Int. 2025;135(1):156–165.
Sun G, Eisenbrey JR, Smolock AR, et al. Percutaneous Microwave Ablation Versus Cryoablation for Small Renal Masses ≤4 Cm: 12-Year Experience. J Vasc Interv Radiol. 2024;35(6):865–873.
McClure T, Lansing A, Ferko N, et al. A Comparison of Microwave Ablation and Cryoablation for RCC: Systematic Review and Meta-Analysis. Urology. 2023;180:1–8.
Schaarschmidt BM, Zensen S, Kesch C, et al. Current Use of Percutaneous Ablation in Renal Tumors: Analysis of the DeGIR Registry. Eur Radiol. 2025;35(3):1723–1731.
Krieger JR, Lee FT, McCormick T, et al. Microwave Ablation of Renal Cell Carcinoma. J Endourol. 2021;35(S2):S33–S37.
Bhagavatula SK, Tuncali K, Shyn PB, et al. Percutaneous CT- and MRI-Guided Cryoablation of cT1 RCC: Intermediate- to Long-Term Outcomes in 307 Patients. Radiology. 2020;296(3):687–695.
Morkos J, Porosnicu Rodriguez KA, Zhou A, et al. Percutaneous Cryoablation for Stage 1 RCC: Outcomes From a 10-Year Prospective Study. Radiology. 2020;296(2):452–459.
Breen DJ, King AJ, Patel N, Lockyer R, Hayes M. Image-Guided Cryoablation for Sporadic RCC: 3- and 5-Year Outcomes in 220 Biopsy-Proven Patients. Radiology. 2018;289(2):554–561.
Cazalas G, Klein C, Piana G, et al. Multicenter Comparative Matched-Pair Analysis of Percutaneous Ablation and Robotic PN for T1b RCC (AblatT1b). Eur Radiol. 2023;33(9):6513–6521.
Michailidis A, Kosmoliaptsis P, Makri D, et al. Percutaneous Cryoablation of T1b Renal Tumors: Local Control, Renal Function, and Ablation Margins in 80 Patients. J Vasc Interv Radiol. 2025. doi:10.1016/j.jvir.2025.09.025.
Abdelsalam ME, Awad A, Kang F, et al. Percutaneous Cryoablation of Clinical T1b Renal Tumors: A Tertiary Cancer Center Experience. Cardiovasc Intervent Radiol. 2026. doi:10.1007/s00270-026-04381-y.
Luzzago S, Mistretta FA, Mauri G, et al. Thermal Ablation for Small Renal Masses: Identifying the Most Appropriate Tumor Size Cut-Off. Urol Oncol. 2022;40(12):537.e1–537.e9.
Gervais DA, McGovern FJ, Arellano RS, McDougal WS, Mueller PR. Radiofrequency Ablation of RCC: Part 1, Indications, Results, and Role Over 6-Year Period and 100 Tumors. AJR. 2005;185(1):64–71.
Rivero JR, De La Cerda J, Wang H, et al. Partial Nephrectomy Versus Thermal Ablation for cT1 Renal Masses: Systematic Review and Meta-Analysis of >3,900 Patients. J Vasc Interv Radiol. 2018;29(1):18–29.
Yang Q, Meng F, Li K, et al. Safety and Efficacy of Thermal Ablation for Small Renal Masses in Solitary Kidney: Meta-Analysis of Comparative Studies. PLoS One. 2015;10(6):e0131290.
Rose TL, Kim WY. Renal Cell Carcinoma: A Review. JAMA. 2024;332(12):1001–1010.
Full technique in RadCall Pro
Probe placement templates by tumor size and geometry, ice-ball tables by probe type, pyeloperfusion flow rates, modality selection algorithm by RENAL score, and sedation protocols available in RadCall Pro.