Calcification Morphology
| Type | Example | Morphology | Malignancy Risk | Action |
|---|---|---|---|---|
| TYPICALLY BENIGN | ||||
| Skin (dermal) | 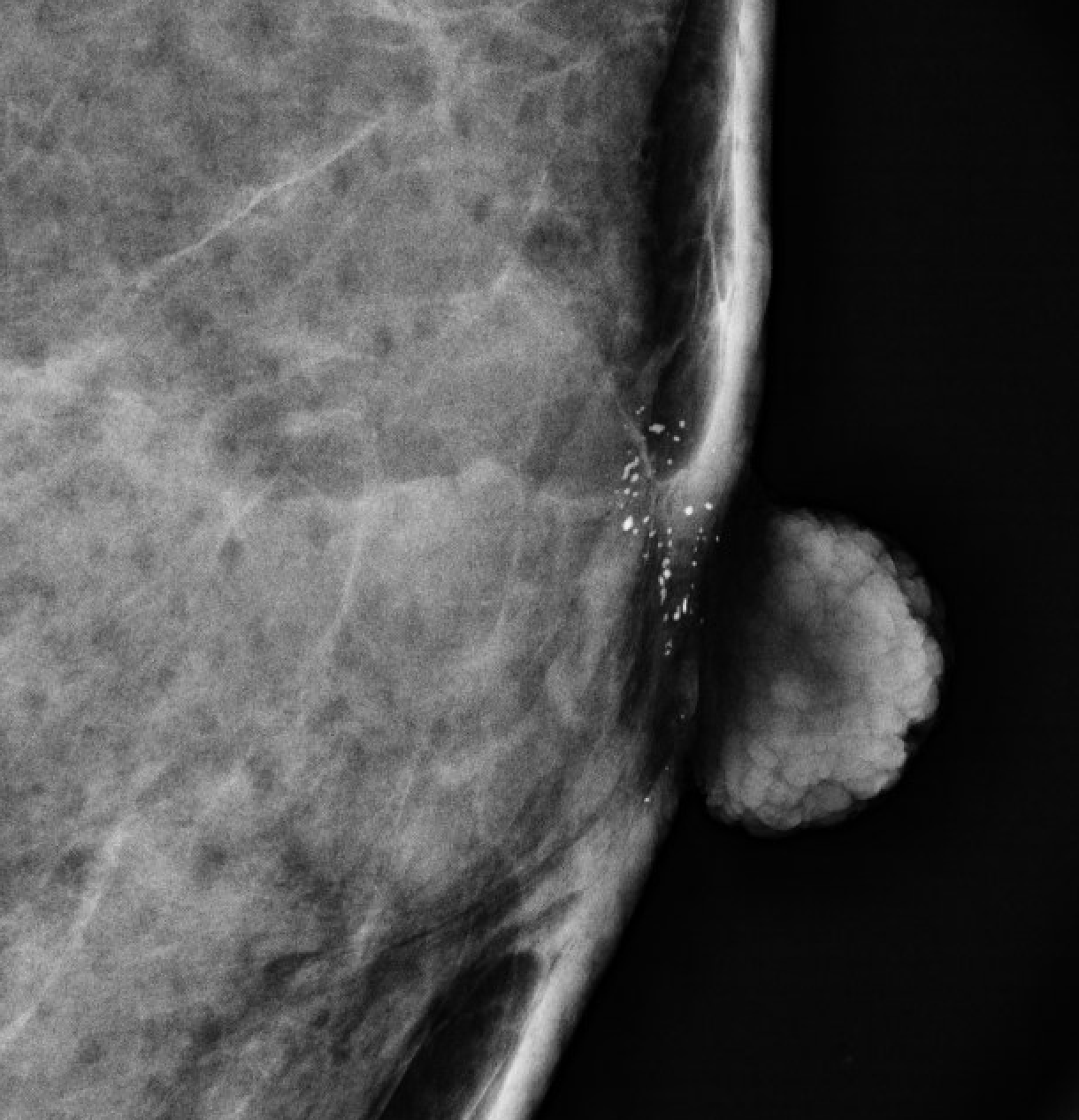 |
Lucent center, polygonal; tangential view confirms skin location | ~0% | BI-RADS 2 |
| Vascular | 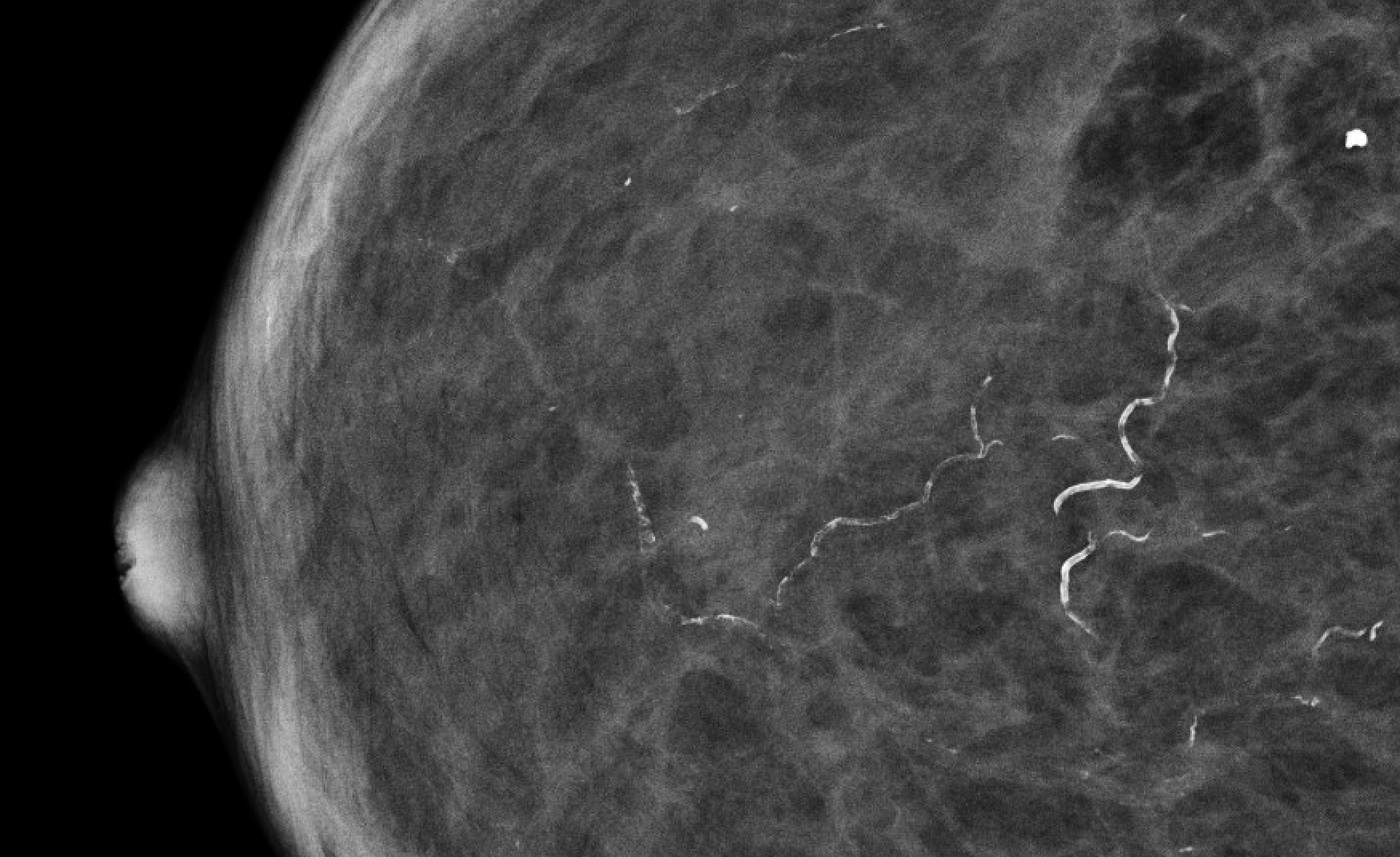 |
Parallel tracks along vessel wall ("tram-track") | ~0% | BI-RADS 2 |
| Coarse / "Popcorn" | 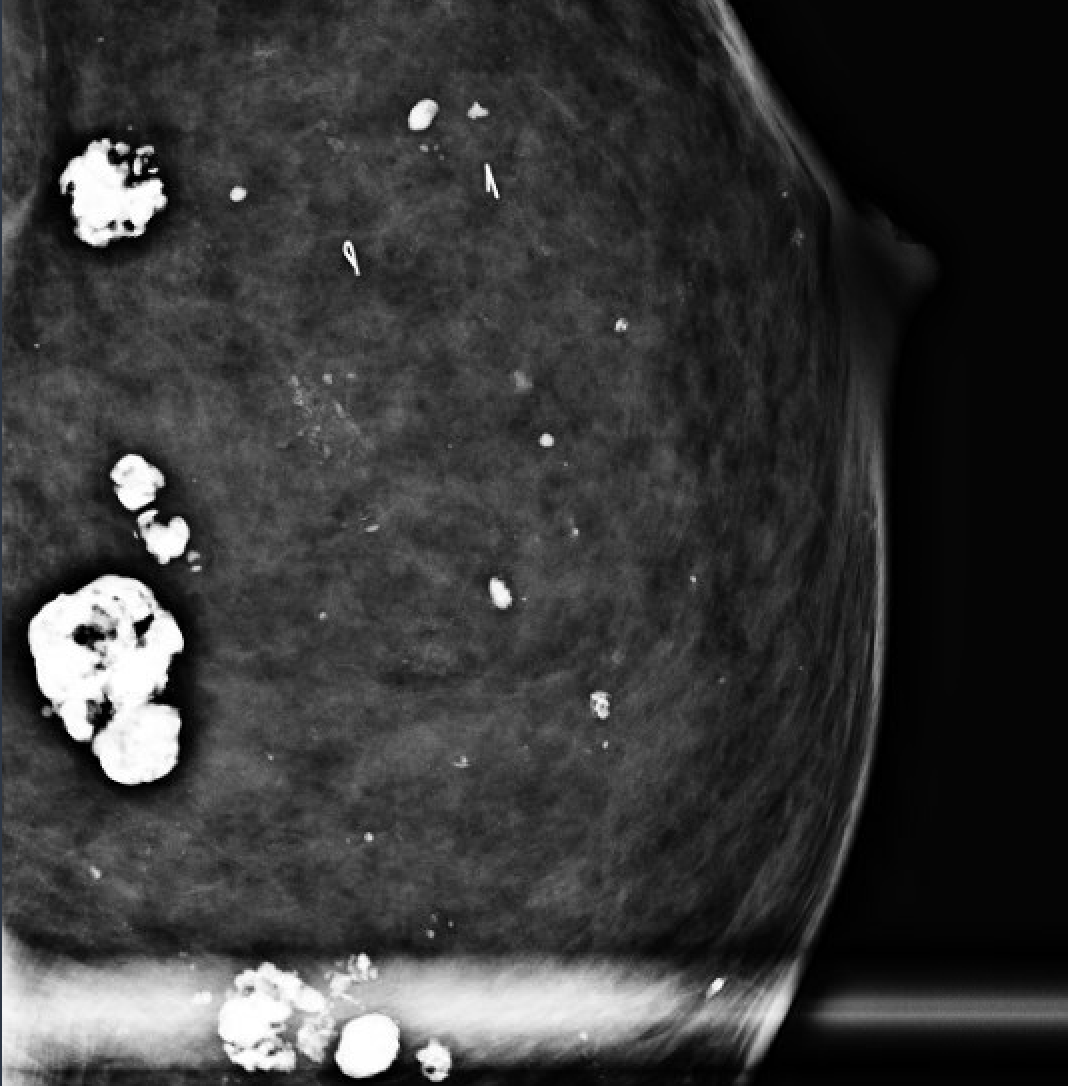 |
Large (>2–3 mm), coarse, central lucency — involuting fibroadenoma | ~0% | BI-RADS 2 |
| Large rod-like (secretory) | 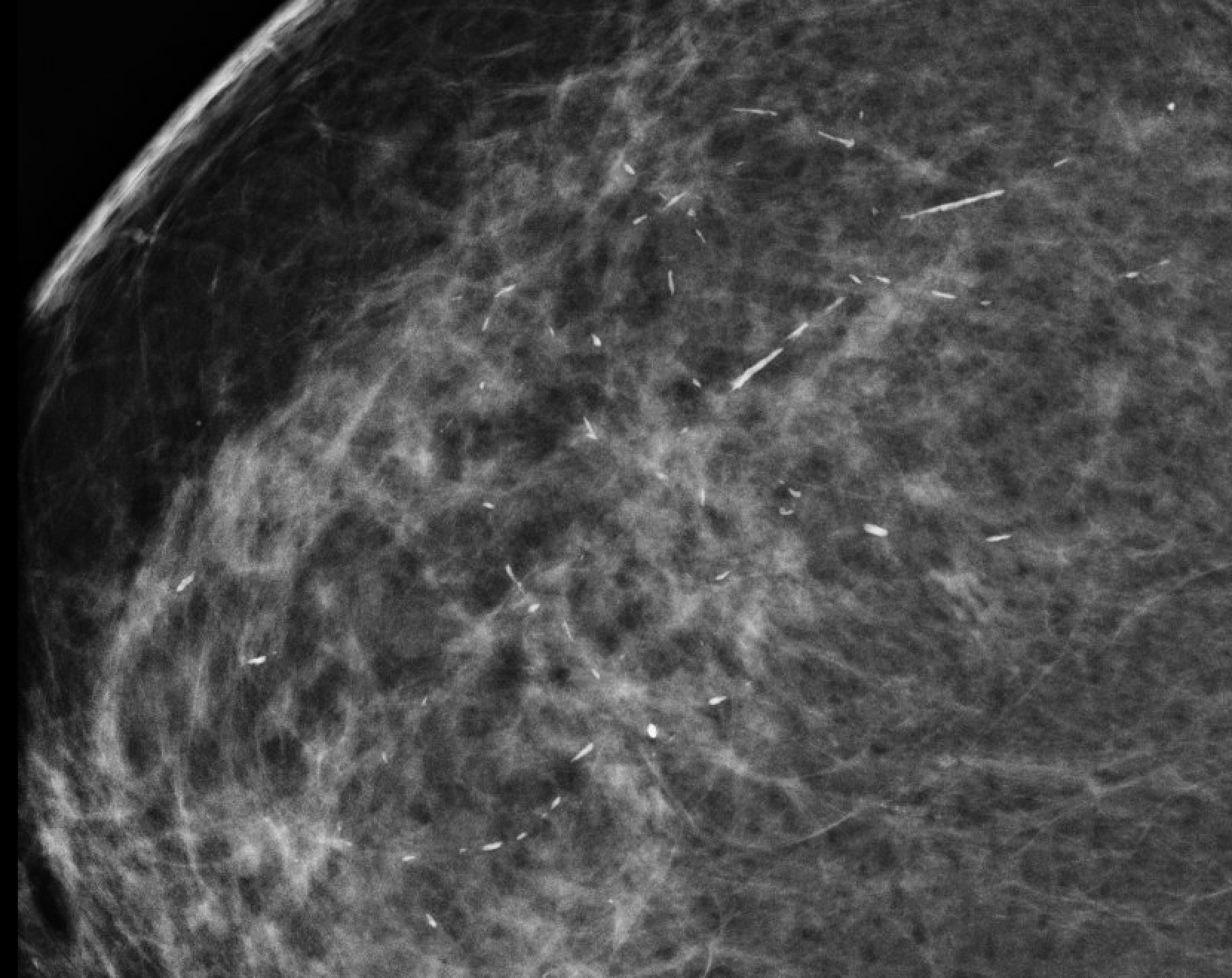 |
≥1 mm rods, may branch, follow duct axis, hollow center | ~0% | BI-RADS 2 |
| Round | 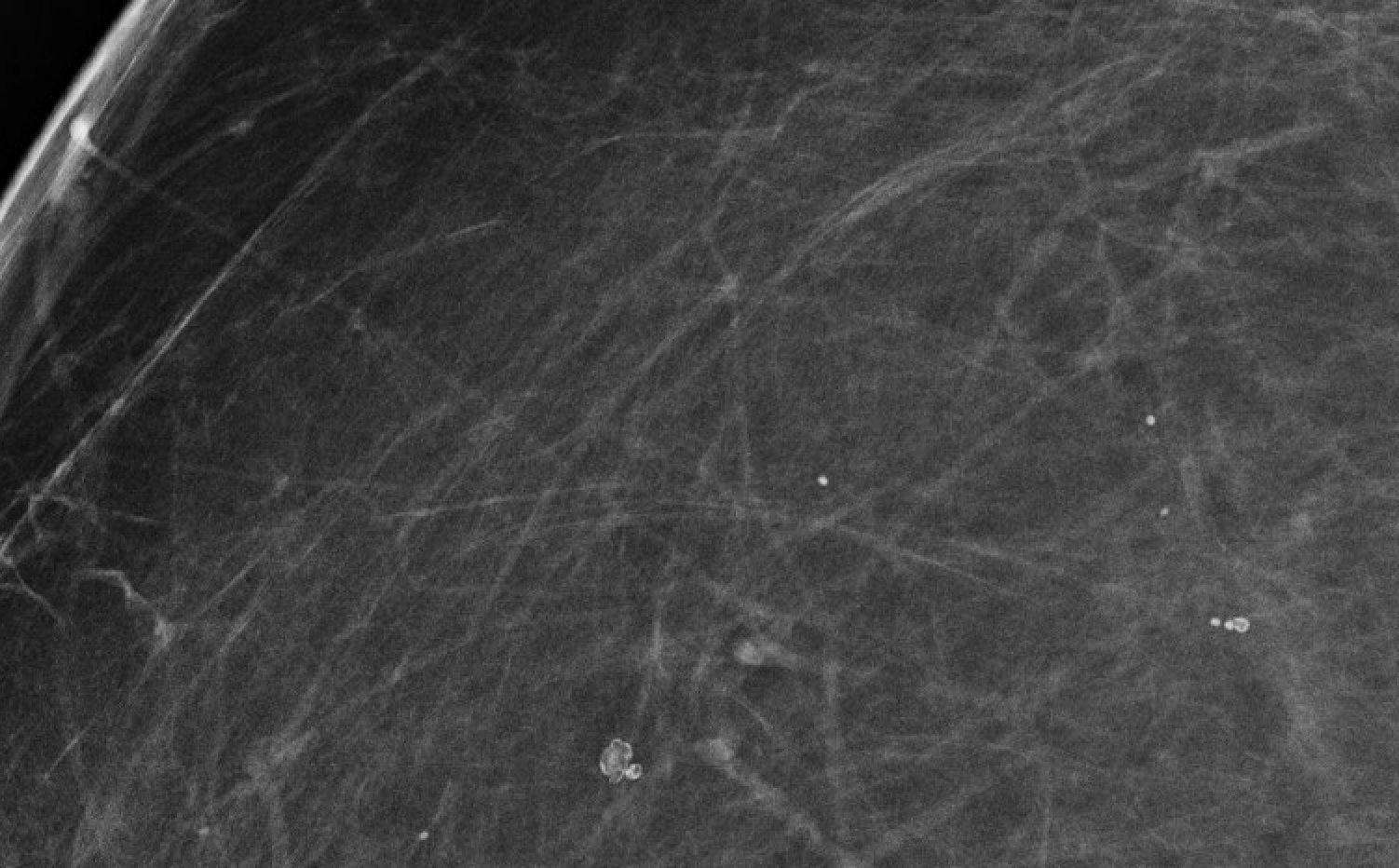 |
≥0.5 mm spheres; bilateral/diffuse = benign; if <0.5 mm = amorphous category | ~0% | BI-RADS 2 if clearly benign context |
| Rim (eggshell / lucent-centered) | 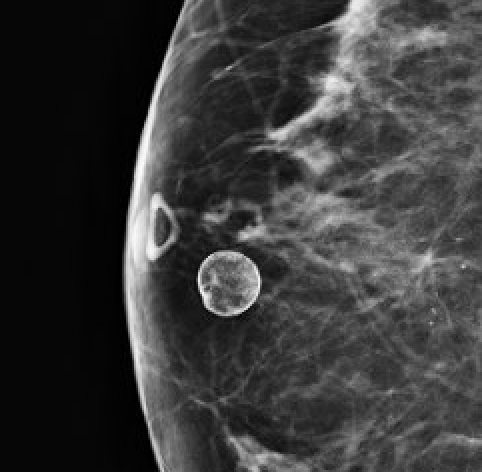 |
Thin shell of calcium around fat — oil cyst, fat necrosis | ~0% | BI-RADS 2 |
| Dystrophic | 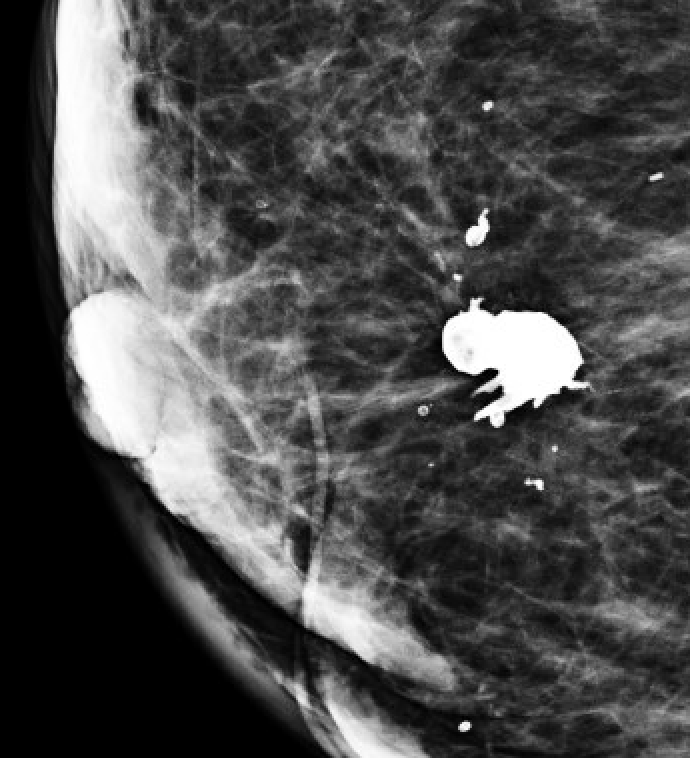 |
Coarse, irregular, >0.5 mm; post-surgical or irradiated breast | ~0% | BI-RADS 2 |
| Milk of calcium | 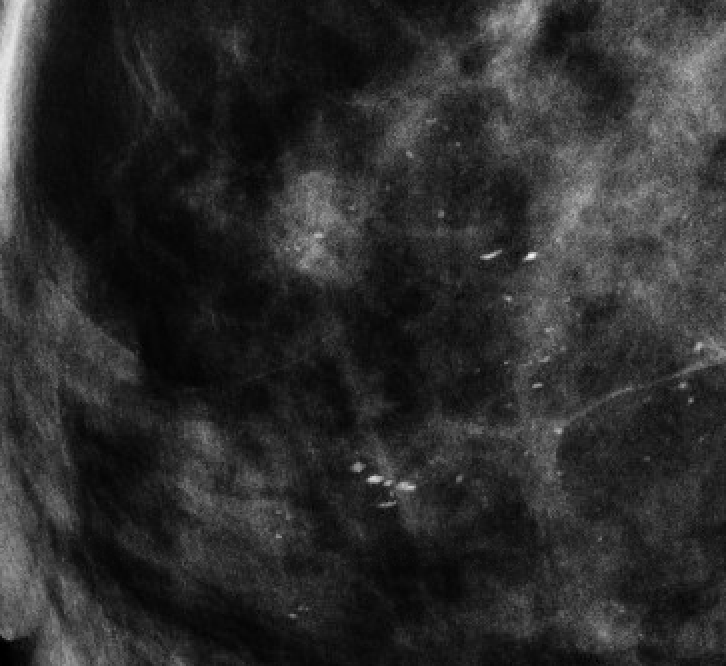 |
Layers dependently on true lateral (crescent/teacup shape); smudged on CC view | ~0% | BI-RADS 2 |
| Suture | 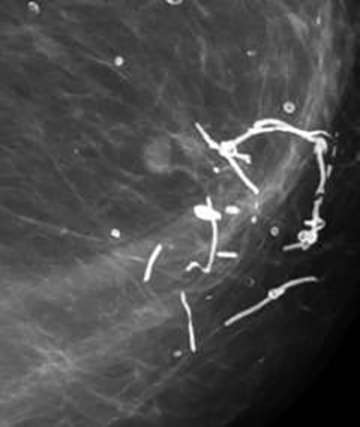 |
Linear/tubular, knot visible; post-surgical history | ~0% | BI-RADS 2 |
| SUSPICIOUS | ||||
| Amorphous | 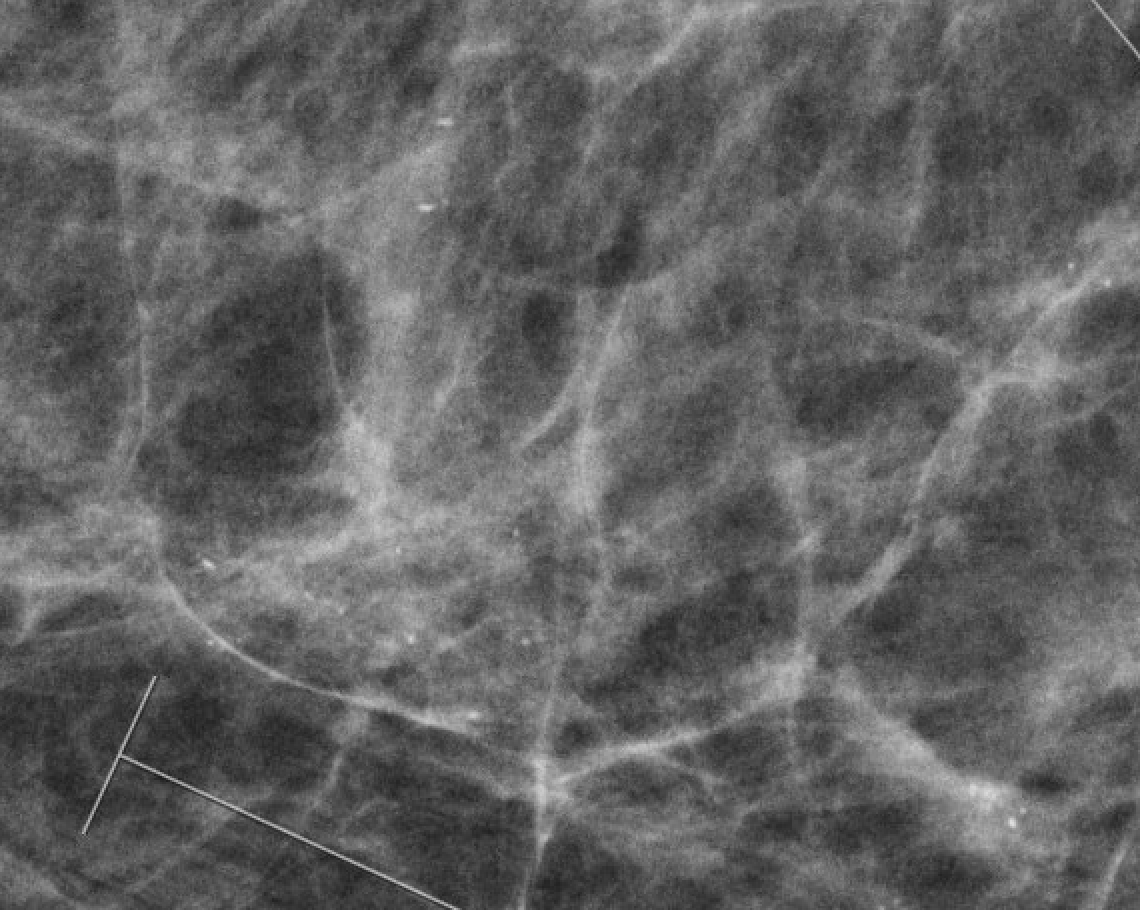 |
Hazy, ill-defined, too small to characterize (<0.5 mm); bilateral diffuse = BI-RADS 3 | ~20% | BI-RADS 4A–4B; biopsy if grouped |
| Coarse heterogeneous | 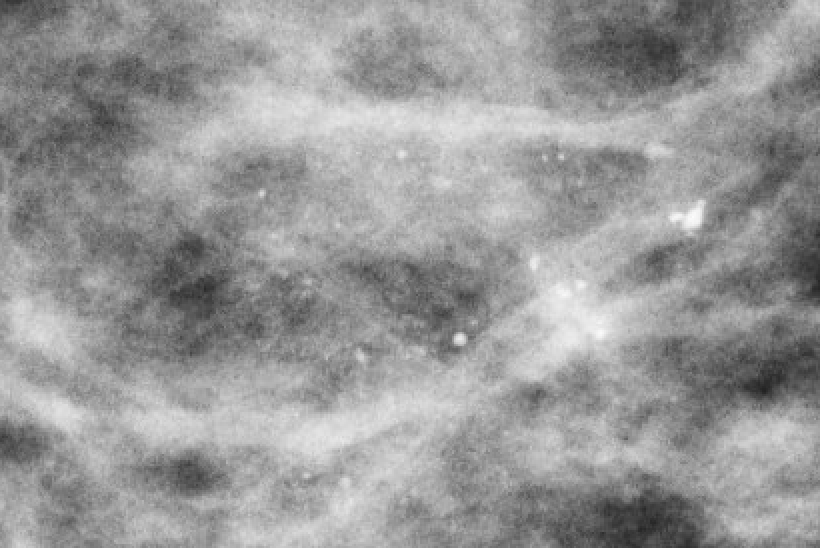 |
Irregular, >0.5 mm; not classic benign types; may coalesce | ~15% | BI-RADS 4B |
| Fine pleomorphic | 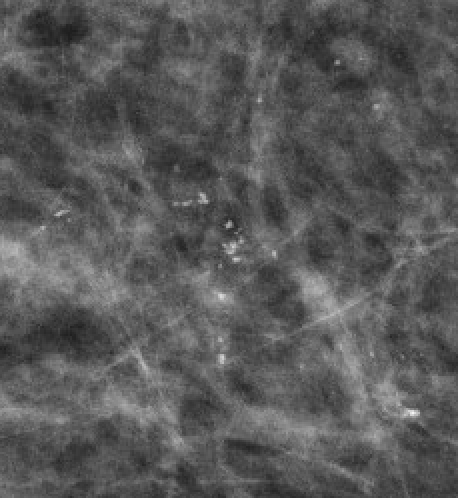 |
Varied shapes and sizes, <0.5 mm; more conspicuous than amorphous | 25–40% | BI-RADS 4B–4C |
| Fine linear / linear branching ("casting") | 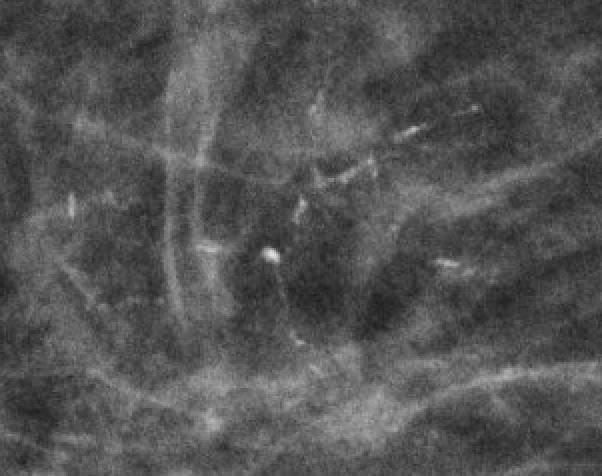 |
Thin (<0.5 mm), irregular, filling duct lumens; branching pattern | ~70% | BI-RADS 4C–5; highest suspicion |
Calcification Distribution
| Distribution | Description | Significance |
|---|---|---|
| Diffuse | Scattered randomly throughout the entire breast — no focal clustering | Typically benign — bilateral diffuse pattern = benign etiology |
| Regional | Occupy >2 cc volume but not a ductal distribution; may involve most of a quadrant | Intermediate — morphology determines action |
| Grouped / Clustered | ≥5 calcifications occupying <1 cc of tissue | Suspicious if fine morphology (amorphous, pleomorphic, linear) |
| Linear | Arrayed in a line — may branch; suggests ductal deposition | Raises concern for ductal malignancy; BI-RADS ≥4 |
| Segmental | In a duct and its branches — triangular/cone-shaped toward nipple | Highest suspicion — implies extensive ductal involvement (DCIS) |
Segmental distribution + fine linear/branching morphology = BI-RADS 4C–5. This pattern is the imaging hallmark of extensive DCIS. Even amorphous calcifications in a segmental distribution require biopsy.
Technique: Always obtain magnification views for calcification characterization when morphology is uncertain on standard views. True lateral views are essential to identify milk of calcium (layering on lateral, smudged on CC). DBT does NOT replace magnification views for calcification workup.