Acute Body MRI — On-Call Hepatobiliary, Pancreatic, Bowel, Renal, and OB/GYN Emergencies
On-call body MRI interpretation: choledocholithiasis, gangrenous cholecystitis, bile leak, pancreatitis, bowel emergencies, pyelonephritis, renal infarct, ectopic pregnancy, ovarian torsion, placental abruption, and postpartum hemorrhage MRI findings.
Quick summary
On-call body MRI interpretation organized by organ system — hepatobiliary, pancreatic, bowel/peritoneal, renal/GU, and OB/GYN emergencies.
Hepatobiliary Emergencies
Condition
Key MRI Findings
Tips
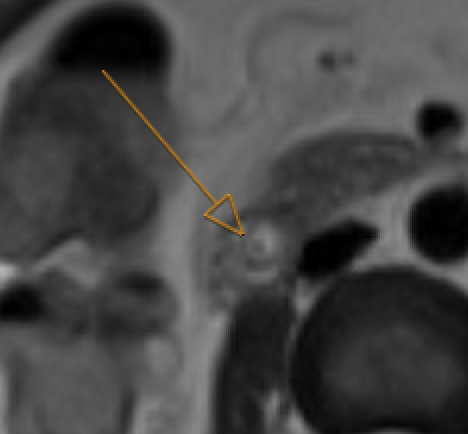
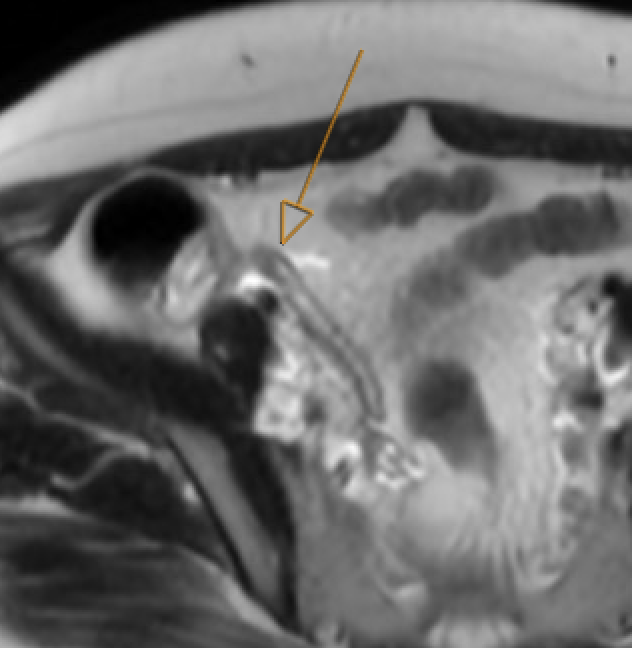
Choledocholithiasis
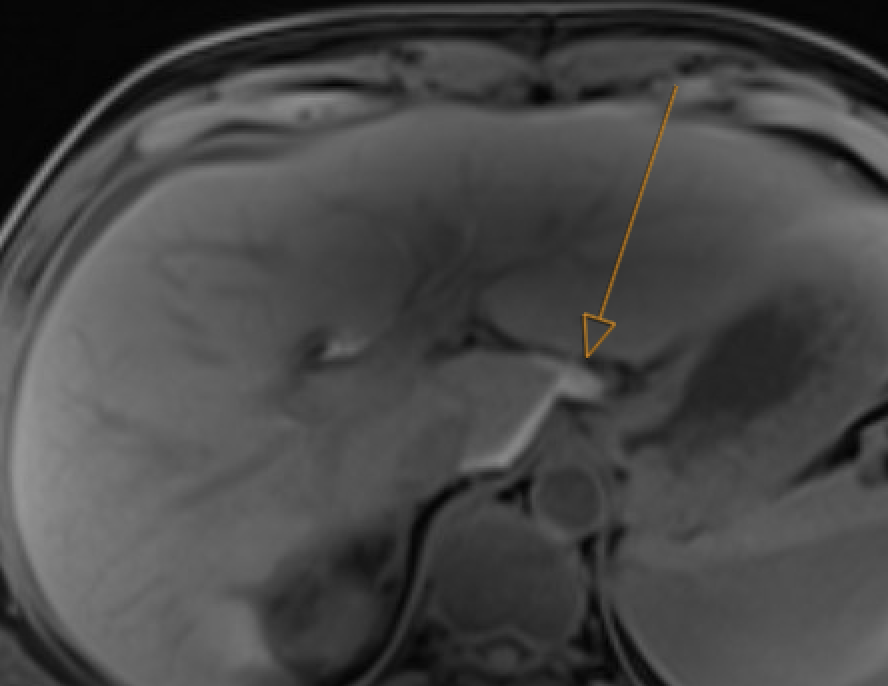
T2-hypointense filling defect in bile duct on MRCP. Obstructive: upstream dilatation, abrupt caliber change. Trace entire biliary system on thin MRCP/T2W
Choledocholithiasis: T2-dark filling defect (arrow) on MRCP
GB neck and cystic duct are blind spots. Pneumobilia can mimic calculi (nondependent, blooms on GRE). Crossing vessel on coronal MRCP can mimic filling defect — check axial reformats
Abscess: rim enhancement + central DWI restriction. Hematoma: central DWI restriction but no rim enhancement + T1 hyperintensity
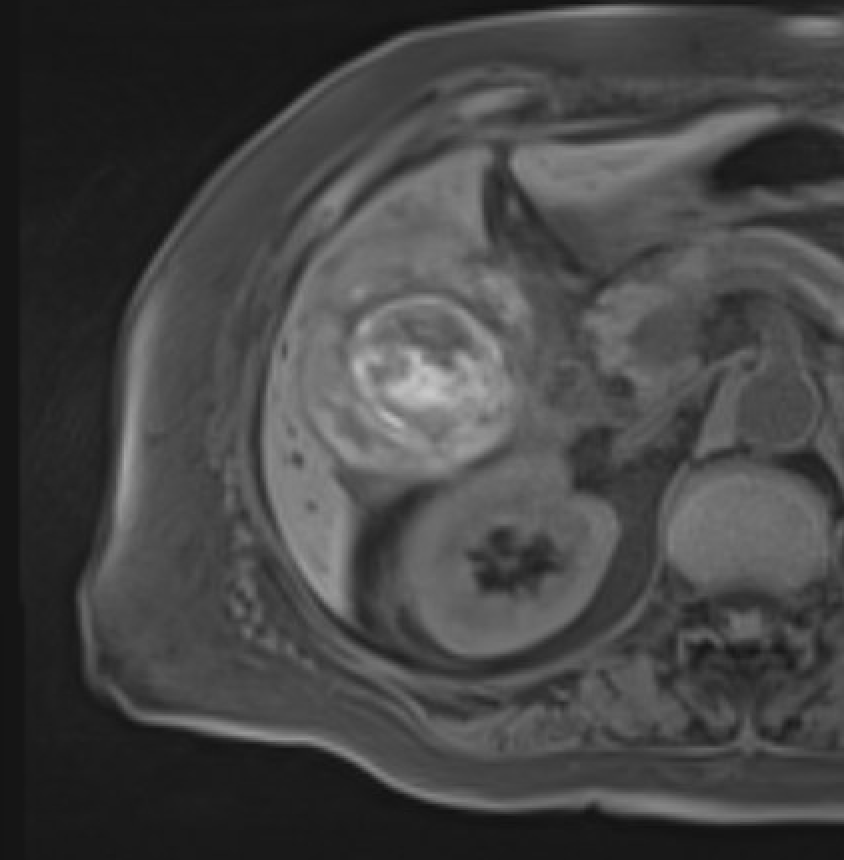
Hemorrhagic cholecystitis
Distended GB with T1-hyperintense and T2-hypointense contents; blooming on T2* GRE; active bleed on subtraction images. No enhancement within hematoma itself
T1W: hyperintense blood products
Both hemorrhage and inspissated bile are T1-bright — use GRE blooming to distinguish. Check subtraction images for active extravasation
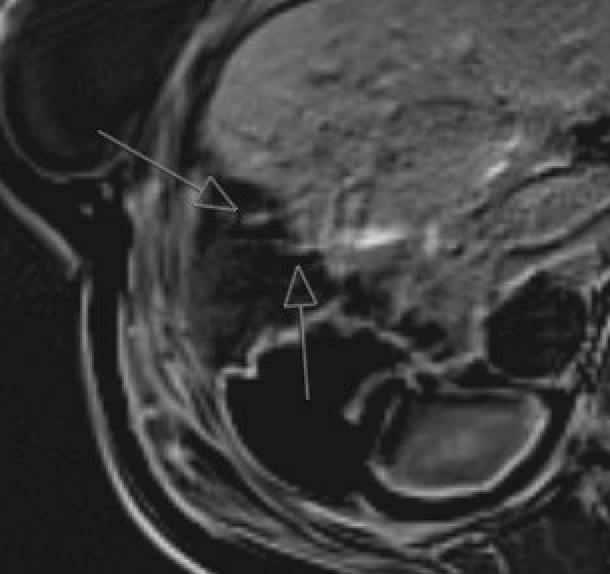
Bile leak / biloma
T2W MRCP: delineate anatomy. Gadoxetate (Eovist) hepatobiliary phase: extravasation of excreted contrast from duct into collection. Add 60–90 min delayed phase if 20–30 min scan is negative
20 min HBP: leak site identifiedDelayed: extravasation confirmed
Avoid gadoxetate if bilirubin >3 mg/dL, severe hepatic failure, or competing drugs (methotrexate, tamoxifen, cisplatin)
Hepatic abscess
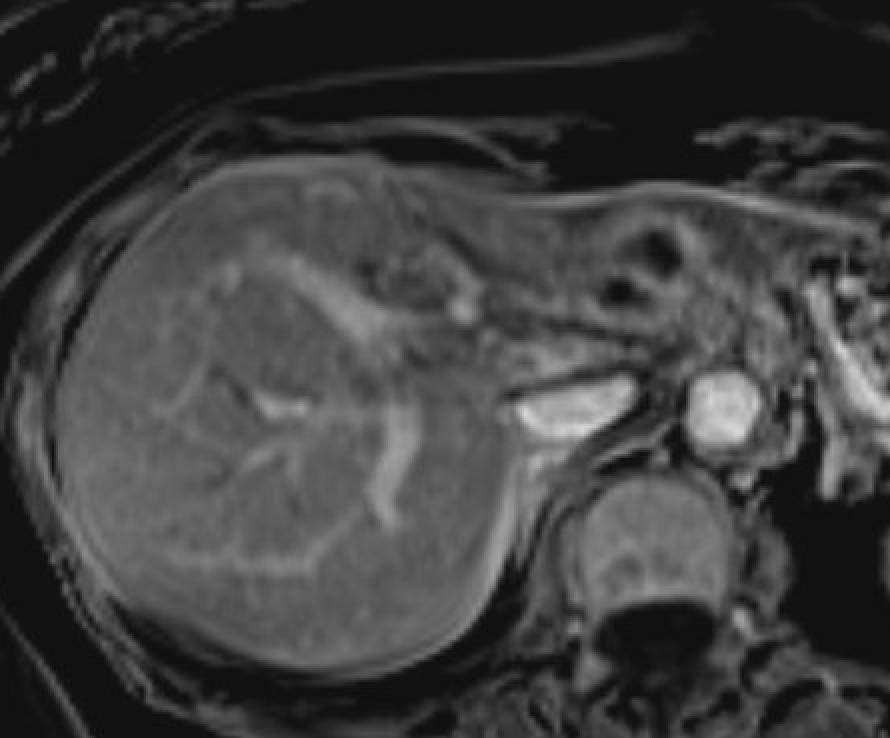
Rim-enhancing collection + central diffusion restriction; double-target sign; perilesional hyperemia (arterial phase)
Hepatic abscess: rim enhancement
Overlaps with cystic metastases — abscess favored by clinical context (fever, leukocytosis, recent biliary intervention). Short-term follow-up if unclear
Hemorrhagic hepatic lesion
Lesion with T1-hyperintense and T2-hypointense blood products; blooming on GRE; nonenhancing hemorrhagic component on subtraction. Look for enhancing viable tumor around hematoma
HCC: check for tumor-in-vein (thrombus enhances like primary tumor). Adenoma: young women, OCP use, peripheral enhancement pattern. Subtraction mandatory when T1 hyperintensity is present
Quick Reference: Peliosis Hepatis vs. Hepatic Abscess
⚠ Critical safety note: Misdiagnosing peliosis hepatis (PH) as abscess and performing percutaneous drainage can cause life-threatening hemorrhage from the blood-filled sinusoidal cavities. When imaging is equivocal, biopsy (transjugular preferred) rather than drainage.
Feature
Peliosis Hepatis
Hepatic Abscess
Clinical
Usually incidental/asymptomatic (70–92%); known associated condition (malignancy, steroids, OCP, immunosuppression, HIV). Normal or mildly elevated LFTs. No fever.
The combination of no DWI restriction + progressive delayed fill-in + ill-defined margins + asymptomatic patient = peliosis until proven otherwise. The combination of restricted diffusion + persistent rim + perilesional edema + fever/leukocytosis = abscess.
A unique overlap entity: bacillary peliosis (Bartonella henselae in HIV/AIDS) can present with fever and elevated ALP mimicking abscess — but shows the vascular fill-in pattern of PH. Responds to erythromycin or doxycycline.
Management
Abscess suspected: Image-guided aspiration for culture ± drainage
Equivocal: Transjugular biopsy preferred over percutaneous (lower hemorrhage risk given vascular nature of PH)
Pancreatic Emergencies
Condition
Key MRI Findings
Tips
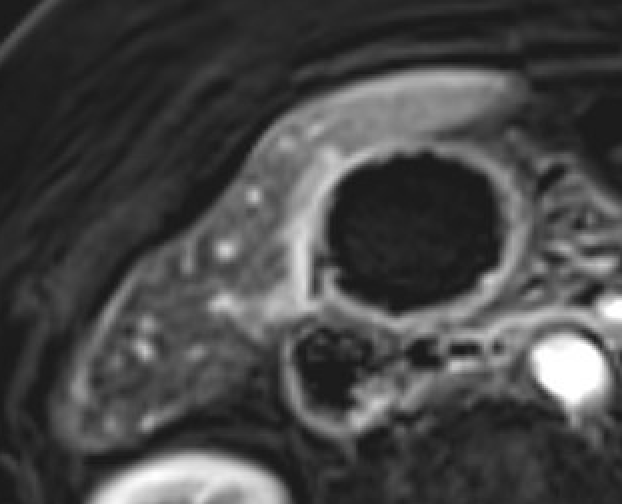
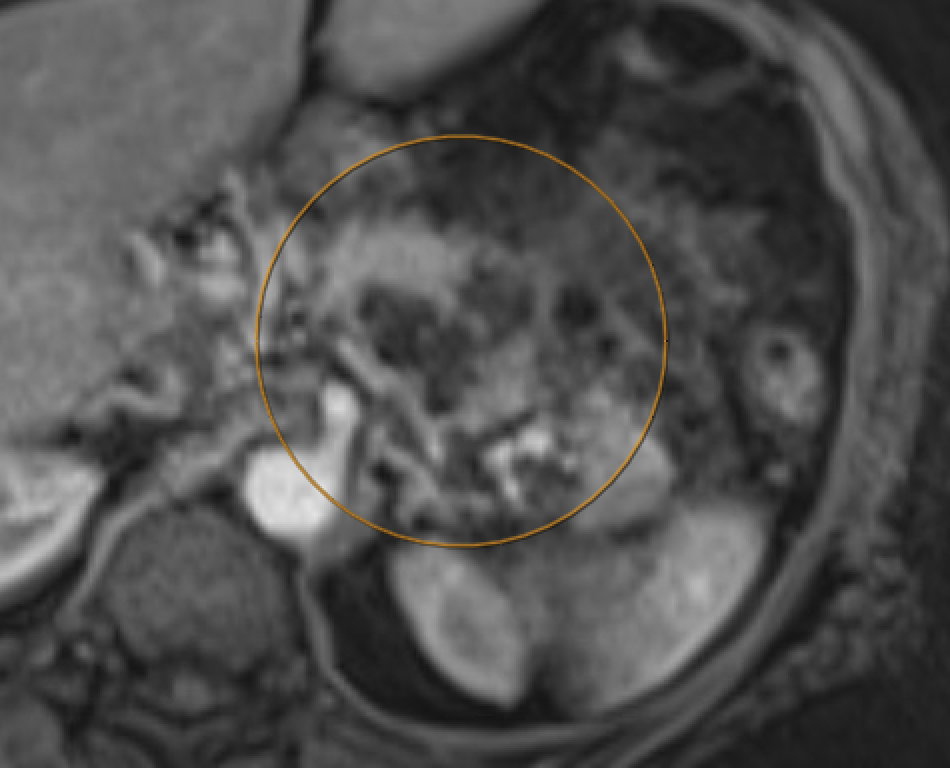
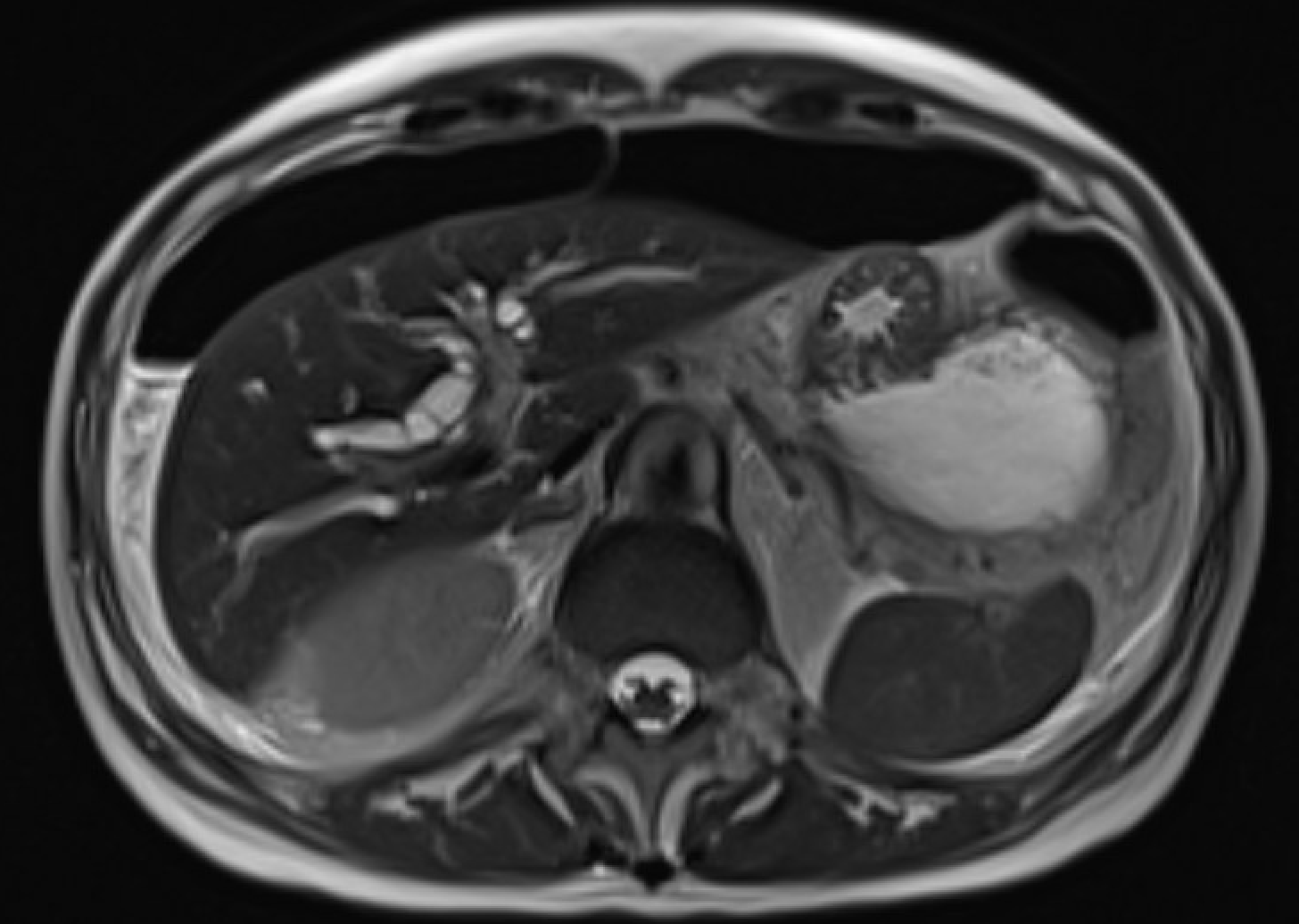
Acute interstitial edematous pancreatitis
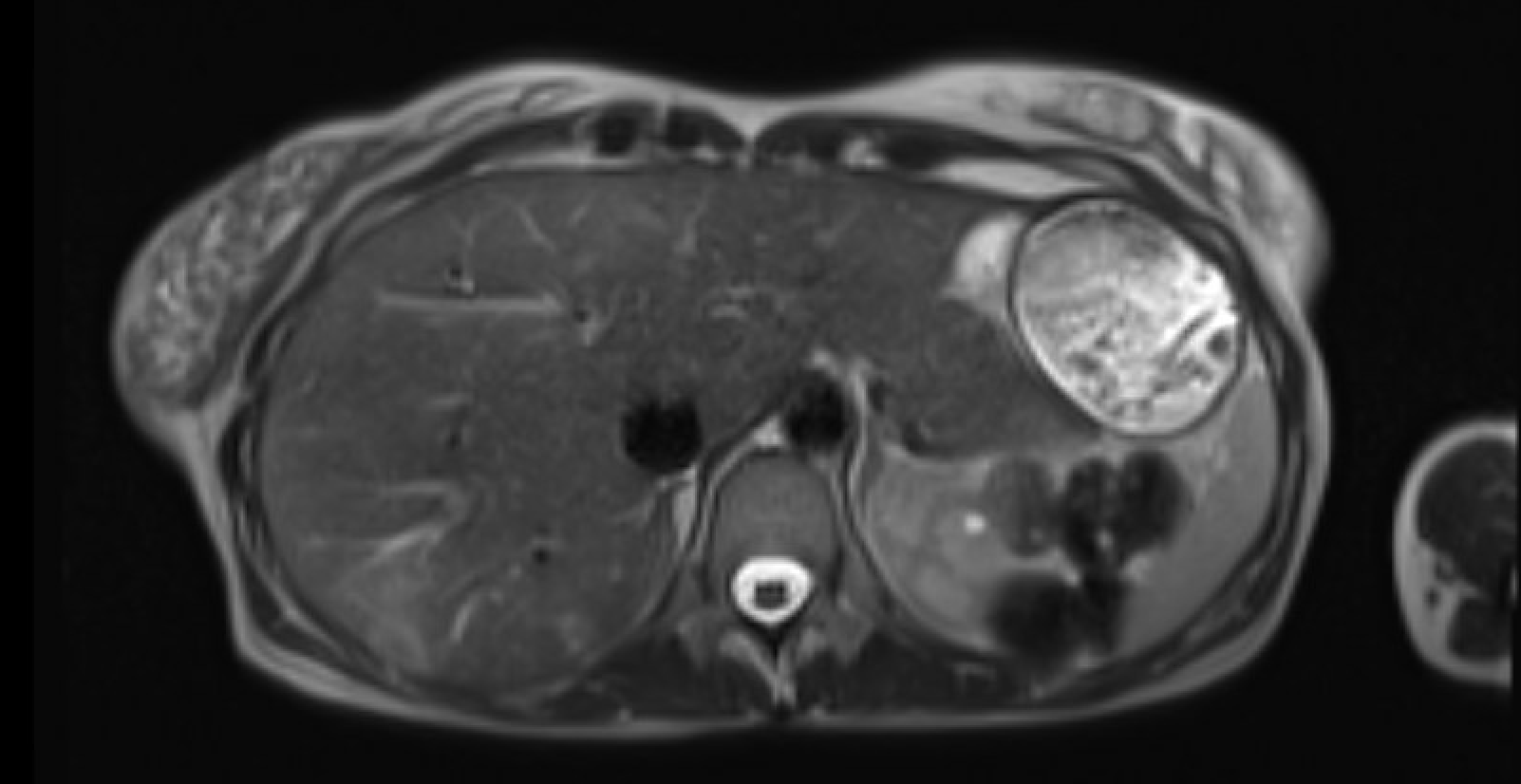
Pancreatic edema (loss of normal T1 hyperintensity) + peripancreatic fluid on T2W + preserved parenchymal enhancement on post-Gd
IEP: loss of T1 signal, preserved enhancement, peripancreatic fluid
Normal pancreas is T1-bright (brighter than liver). Loss of T1 signal = edema/inflammation. DWI restriction is sensitive for early pancreatitis. India ink artifact on out-of-phase shows subtle fat stranding
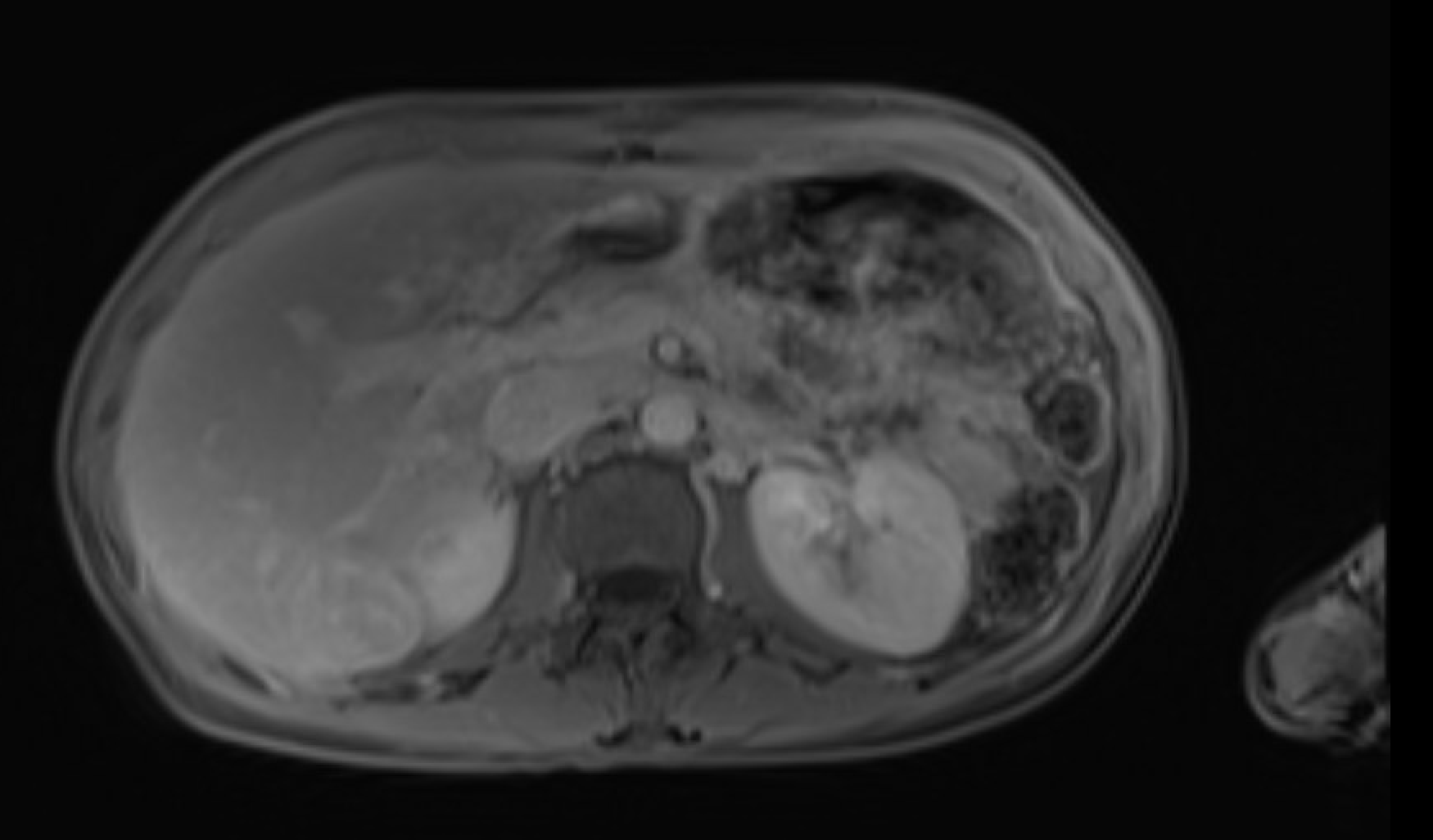
Acute necrotizing pancreatitis
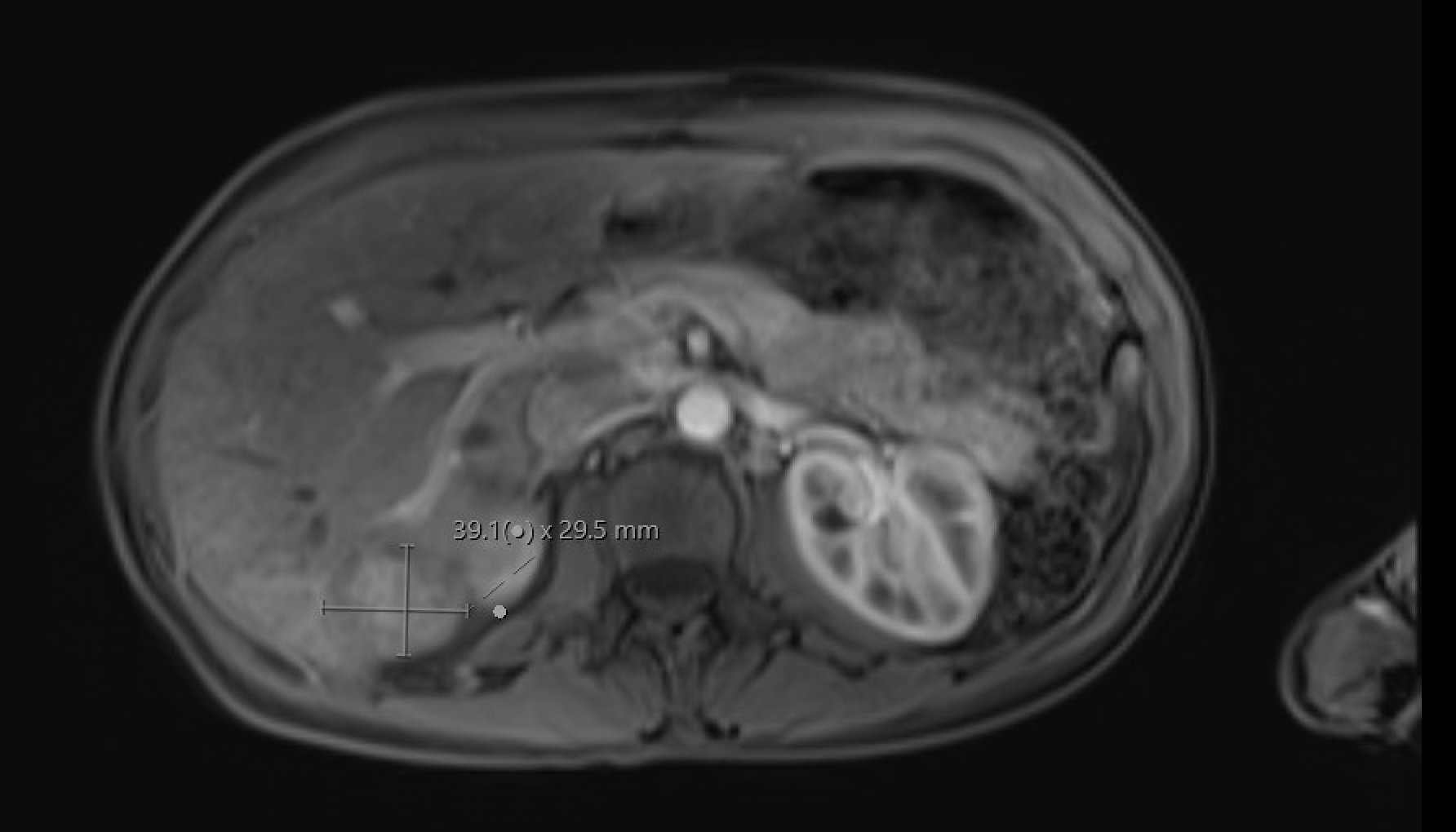
Lack of parenchymal enhancement on post-Gd = necrosis. Hemorrhage: T1 hyperintensity + GRE blooming. Vascular complications: thrombosis (filling defect on bSSFP/post-Gd), pseudoaneurysm
Necrotizing pancreatitis: nonenhancing parenchyma = necrosis
Pitfall: Diffuse hemorrhagic necrosis can appear T1-bright, mimicking normal pancreas. Always check post-Gd for absent enhancement and T2W for necrosis
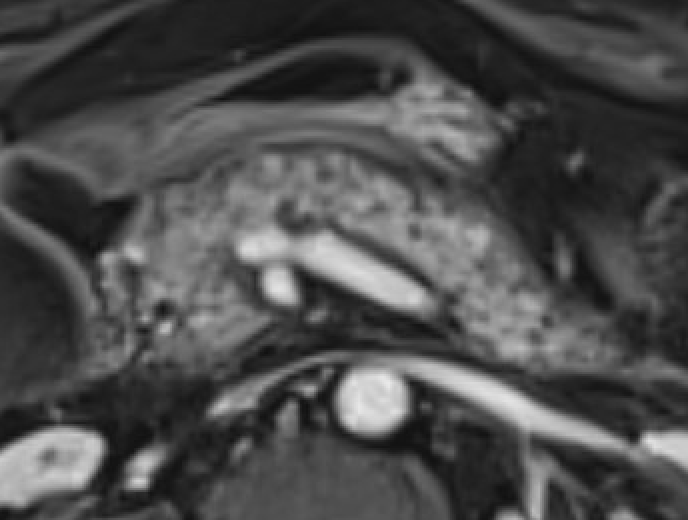
Pancreatic trauma
Full-thickness laceration = T2-hyperintense linear signal disrupting parenchyma. Trace pancreatic duct on T2W axial images (MRCP often limited by surrounding fluid)
Ductal injury (AAST Grade III+) = surgical indication. MRI better than CT for delineating duct integrity. Contusions (Grade I/II) without duct injury → conservative
Bowel & Peritoneal Emergencies
Condition
Key MRI Findings
Appendicitis (pregnancy)
Dilated appendix ≥7 mm, wall thickness >2 mm, periappendiceal fluid/fat stranding on T2W. Appendicolith: T2-hypointense filling defect (confirm on bSSFP). Appendix migrates cranially with gestational age. Sensitivity 94%, specificity 97%
Appendicitis: dilated appendix, periappendiceal stranding
Diverticulitis
Colonic wall thickening >3 mm with diverticula; pericolic fat stranding on T2W FS; abscess: rim-enhancing + DWI-restricting collection. MRI sensitivity 86–94%, specificity 88–92%. Better soft-tissue resolution for fistula, oophoritis
Diverticulitis: wall thickening, pericolic T2 stranding
Crohn complications
Stricture: wall thickening >3 mm + luminal narrowing >50% + upstream dilatation. Penetrating: sinus tract, fistula, phlegmon, abscess (rim enhancement + DWI restriction). Active inflammation: wall edema + hyperenhancement on T2W FS and post-Gd
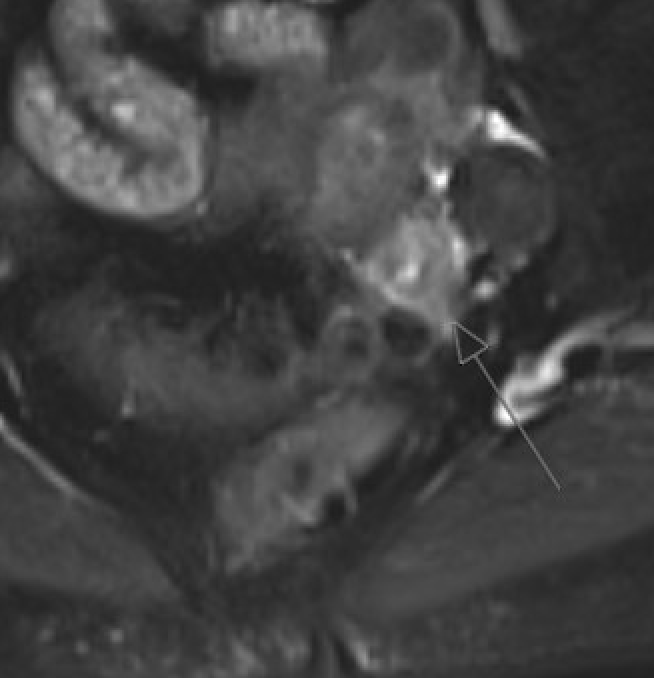
Perianal fistula
Small-FOV T2W FSE along anal canal is key. Report: tract type (Parks classification — intersphincteric / transsphincteric / suprasphincteric / extrasphincteric), internal and external openings, branches, abscess. DWI + post-Gd for abscess vs granulation vs fibrosis
Perianal fistula: T2W tract, internal opening, sphincter relation
Pneumoperitoneum
Subtle T2-hypointense foci in peritoneal cavity. Air-fluid levels. Susceptibility artifact on bSSFP and T1W GRE sequences. Can be easily missed — look for abnormal extraenteric T2-dark foci
Pneumoperitoneum: T2-dark extraenteric foci, GRE susceptibility
Renal & GU Emergencies
Condition
Key MRI Findings
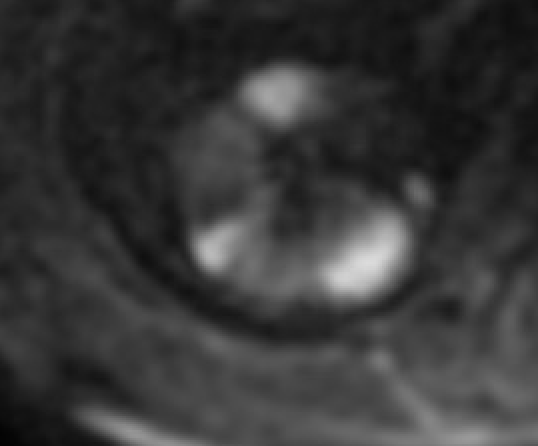
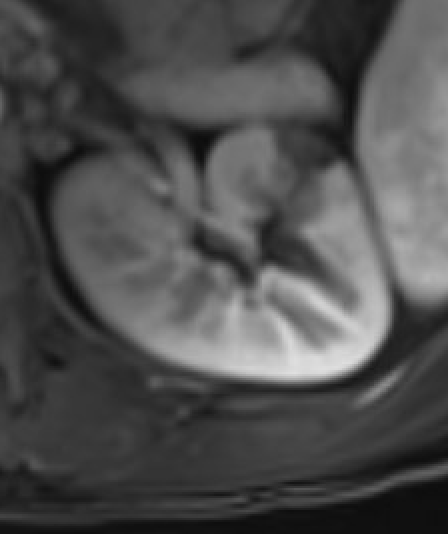
Pyelonephritis
Wedge-shaped T2 hyperintensity with striated nephrogram; wedge-shaped hypoenhancement on post-Gd; wedge-shaped DWI restriction. Abscess: rim-enhancing collection with central DWI restriction
Pyelonephritis: wedge-shaped diffusion restriction
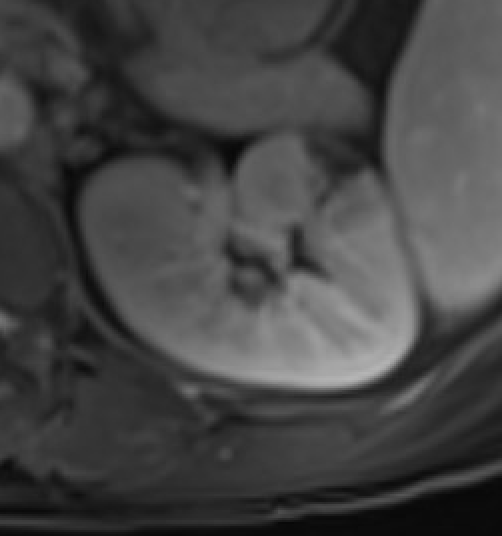
Renal infarct
Wedge-shaped nonenhancement with cortical rim sign (preserved capsular vessel enhancement); cortical DWI restriction
Renal infarct: wedge-shaped nonenhancementDelayed: cortical rim sign
Urolithiasis (pregnancy)
Hypointense filling defect in dilated ureter — better seen on bSSFP than T2W. Distinguish from physiologic hydroureteronephrosis (gradual tapering at pelvic brim, right > left)
Subcapsular/perirenal T1-hyperintense collection with T2 signal heterogeneity. Subtraction images mandatory to exclude underlying enhancing neoplasm (AML, RCC most common causes)
OB/GYN Emergencies
Condition
Key MRI Findings
Placental abruption
Retroplacental or subchorionic hematoma: T1-hyperintense blood products (T1 better than T2 for hemorrhage detection). T2 can underestimate hemorrhage extent. bSSFP may show subchorionic hematoma better than T2
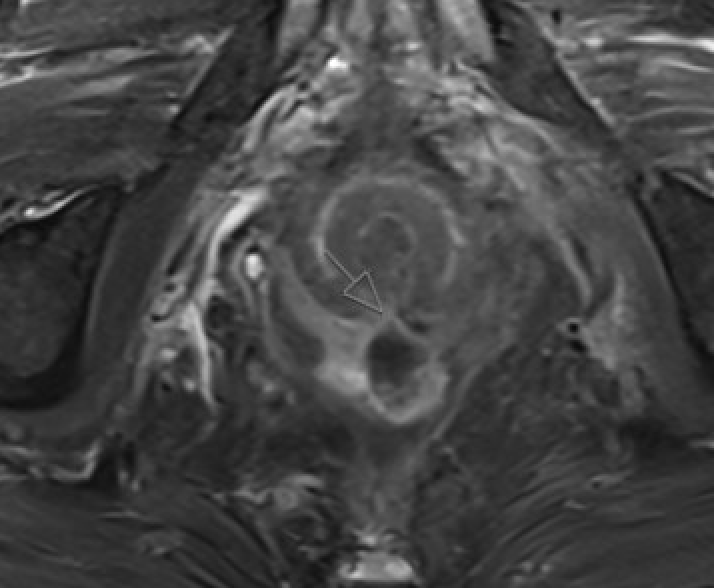
Ectopic pregnancy
Gestational sac outside endometrial cavity on T2W. Locations: tubal (most common), cornual, cervical, cesarean scar. MRI localizes ectopic precisely when US is indeterminate. Cesarean scar ectopic: sac in lower uterine segment scar, residual myometrium <2 mm = rupture risk
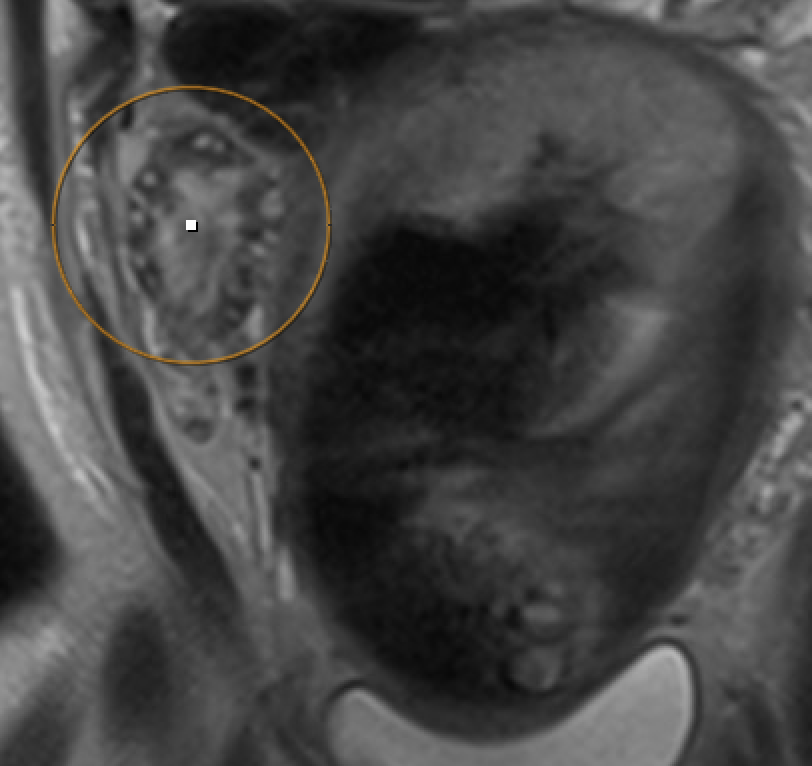
Ovarian torsion (pregnancy)
Enlarged ovary with peripheral follicles and stromal edema on T2W. Pelvic ascites. Compare with contralateral ovary. Whirlpool sign of twisted pedicle
Ovarian torsion: enlarged ovary, peripheral follicles, stromal edema
Postpartum hemorrhage — RPOC vs UVA
RPOC: enhancing endometrial tissue (≤ myometrium = moderate; > myometrium = hypervascular). Serial β-hCG decreases. UVA/AVF: serpiginous flow voids, early draining vein on time-resolved MRA. Low-flow UVA: myometrial blush without early draining vein
MRI in pregnancy: Safe at ≤3 T (prefer 1.5 T in 1st trimester). GBCAs are FDA Class C — avoid unless benefit clearly outweighs risk; use lowest dose of macrocyclic Group II GBCA with informed consent. Non-contrast sequences (T2W SSFSE, DWI, bSSFP, T1W) are sufficient for most acute indications. For renal failure (eGFR <15): Group II GBCAs can be used after risk-benefit discussion; space injections ≥7 days apart.
Reference
Panda A, Aswani Y, Heming CAM, et al. On-Call Body MRI: A Primer. RadioGraphics. 2025;45(1).
More in RadCall
99+ guides, IR procedure playbooks, systematic search patterns, case logging, and wRVU tracking — all in one place.